TH-cam
US
EKG/ECG Interpretation (Basic) : Easy and Simple!
12:24
Are You A Medical Legend? Test Your Knowledge With This Ecg/ekg Quiz! #electrocardiogram
13:09
How to perform a 12 lead ECG
26:08
New Colour Match Puzzle Challenge with Cola and McDonald’s Avengers Logo - Incredibox Sprunki
00:22
【พากย์ไทย】ฮ่องเต้เมาและหลับไปกับนางใน แต่นางในตั้งท้องมังกรทันที จึงได้รับการแต่งตั้งเป็นพระมเหสี
1:07:14
🔴LIVE สด! PGC 2024 ศึกชิงแชมป์โลกพับจี Circuit 3 วันที่ 2
5:17:45
How to Place and Acquire a 12-Lead Diagnostic EKG
Best Practice Medicine
ติดตาม
6K
ดาวน์โหลด
โหลดลิงค์.....
มุมมอง 378 966
0
0
เพิ่มลงใน
เพลย์ลิสต์ของฉัน
ดูภายหลัง
แชร์
แชร์
ฝัง
ขนาดวิดีโอ:
1280 X 720
853 X 480
640 X 360
แสดงแผงควบคุมโปรแกรมเล่น
เล่นอัตโนมัติ
เล่นใหม่
เผยแพร่เมื่อ 2 ก.พ. 2025
ความคิดเห็น • 140
ต่อไป
เล่นอัตโนมัติ
12:24
EKG/ECG Interpretation (Basic) : Easy and Simple!
MINT Nursing
มุมมอง 6M
13:09
Are You A Medical Legend? Test Your Knowledge With This Ecg/ekg Quiz! #electrocardiogram
The Learn Medicine Show
มุมมอง 57K
26:08
How to perform a 12 lead ECG
Royal Wolverhampton NHS Trust
มุมมอง 807K
00:22
New Colour Match Puzzle Challenge with Cola and McDonald’s Avengers Logo - Incredibox Sprunki
FlowerTeam
มุมมอง 3.8M
1:07:14
【พากย์ไทย】ฮ่องเต้เมาและหลับไปกับนางใน แต่นางในตั้งท้องมังกรทันที จึงได้รับการแต่งตั้งเป็นพระมเหสี
Fresh Thailand
มุมมอง 769K
5:17:45
🔴LIVE สด! PGC 2024 ศึกชิงแชมป์โลกพับจี Circuit 3 วันที่ 2
PUBG: BATTLEGROUNDS THAILAND
มุมมอง 169K
53:39
OHANA บ้าพลัง EP.134 : เกมการ์ดโอฮาน่า X วัยหนุ่ม 2544
ohana clip
มุมมอง 662K
16:39
CPR for children video (aged 1-8 years) taught by paediatric nurse Sarah Hunstead
CPR Kids TV
มุมมอง 289K
6:06
Applying Electrodes for a 12 lead EKG - Clinical Nursing Skills | @LevelUpRN
Level Up RN
มุมมอง 43K
14:10
ABCDE Assessment | Sepsis | Emergency Simulation Scenario | OSCE Guide | UKMLA | CPSA | PLAB 2
Geeky Medics
มุมมอง 642K
4:06
How to obtain a 12-lead ECG with proper electrode placement and excellent data quality
Tom Bouthillet
มุมมอง 87K
3:19
CPR in Action | A 3D look inside the body
Action First Aid
มุมมอง 12M
12:52
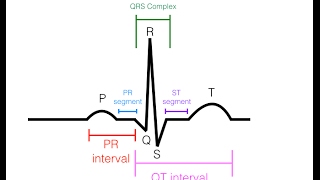
P,Q,R,S,T waves in the EKG
Dr. John Campbell
มุมมอง 1.1M
12:14
Most Common ECG Patterns You Should Know
Rhesus Medicine
มุมมอง 1.7M
1:54:37
12 Lead EKG Interpretation for Paramedic Students. Pass the NREMT with Pass with PASS!
Pass with PASS
มุมมอง 31K
10:05
12 Lead EKG (ECG)
Dr. John Campbell
มุมมอง 830K
58:23
หนูกับเต้ รัก ”พี่อู๋จูน“ นะ
หนูม่วง คำหลู่
มุมมอง 536K
33:22
แมนยู Corner : คุยหลังเกม แมนฯซิตี้ 1-2 แมนฯยู ชัยชนะมาจากอโมริมกล้าตัด แรชฟอร์ด , การ์นาโช
Fluke Family
มุมมอง 274K
1:23:46
【หนังพากย์ไทย】ยอดฝีมือสังหารนักโทษ แต่นักโทษเป็นปรมาจารย์กังฟูที่ซ่อนอยู่ เขาจัดการทั้งหมดในทันที
Fresh Thailand
มุมมอง 468K
14:51
Highlight | อัจฉริยะสาวไส้...เบื้องลึกเหตุยิง "สจ.โต้งปราจีนบุรี" | เปิดโต๊ะข่าว | 17 ธ.ค.67
PPTV HD 36
มุมมอง 390K
00:52
มายคราฟ, แต่ ไลค์ = หัวใจ!
จิน
มุมมอง 296K
55:01
ช้างศึกโดนก่อน ไล่ยิงคืนสิงคโปร์ ทะลุน็อคเอาท์
ฟุตบอล108
มุมมอง 101K
39:39
ใครคือฆาตกรตัวจริง ?! EP.11 (ver. คืนคริสมาสต์ สุดสยอง !!!
Sunflowava
มุมมอง 307K
09:49
#โด่งดัง!ญี่ปุ่นซูฮก บอลอาเซียนเร้าใจ!! โค๊ชสิงคโปร์พูดแบบนี้ถึงไทย!! มาเลย์ขอบคุณไทยที่ให้ชีวิต..?
# จัน ฑาล
มุมมอง 199K