Ive been taking this medication for three years and it has been a lifesaver. I suffered from extreme anxiety, a sense of despair and gloom that no other medication had solved. It has helped enormously. It also helped me with debilitating insomnia. I take 30 mg every night and will likely be on it for the rest of my life. 54 year old male
Wait till you start getting the issues! There highly addictive for one and I kept getting seratonin syndrome and nobody could tell me what the issue was!
@@EMPERORSPROTECTION-TERRA4LIFE no issues at all, nothing but benefits. I know about serotonin síndrome and that hasn’t been a problem. You may have taken something else in addition to mirtazapine to trigger that in the first place
@@pauls4923 😂 not at all! Read everybodies relies about the nightmare they are going through because of this addictive drug and how the doctor ignored the basic question to “explain why we need to wean off a non addictive drug?”. It’s an addictive drug simple as that
@@EMPERORSPROTECTION-TERRA4LIFE it’s a drug that has been a complete and total lifesaver for me and for many others. I don’t care if it’s addictive if it’s going to relieve overwhelming anxiety and depression. Thank God I’ve found it! I’ll be on it til death.
I was prescribed this medication post army, it was great, then plateaued, the doc recently realised i was still on the 15mg, and now has upped it 45mg and i have to say. my everyday life has become SO much more releif for anxitey, focus, mood and apetite. Thank you for your referenece
@@AyeshaKhan-ll7mwmadam man jis bhi video ka neeechy comment karti hon ya parhti hon vahan ap hoti han chahay vo koi British ho indian ho pakistani ho matlab ap bhi meri trha Sara din yahi karti han is ka ilava banda is halat main or kar bhi kia sakta hae 😭😭😭😭😭
@@taqihaider456 G JB Mai ye medicine use kr Rai ti to mai bhi asi hi ho gae ti q k me ne bhttt salo se Ecetelopram use kia ta . Lekin ab mujhe mere Dr ne Raxil Cr dya hai q k Mera weight gain ho Raha ta . AP tention na lo ap kch weeks use kr ly in Sha Allah thk ho jae gi . Or ye time lety hai anti depression tablets so plzz sabr se Kam ly or apny Dr ko follow kry or meditation hai U tube Mai search kr ly foggy brain Anxiety or depression ki kch time kry in Sha Allah bhtt behtr feel kry gi .
Thank you for sharing your knowledge!! I used this for insomnia and severe postpartum depression years ago with great results. Years later I went back on for insomnia and night sweats during menopause. Again with great results, a good nights sleep is finally with no night sweats. Your explanation gave me a clear picture of how the medicine works which no one ever explained before to me. I am off of it now and no withdrawal issues. Thank you again for sharing.
Anna if you dont mind answering, what was your plan for withdrawal and how long were you on Mirtazepine? I am having problems with insomnia and worry about taking an antidepressant just for it, but seriously considering Mirtazepine
You do know that there’s not any proof whatsoever that a chemical imbalance causes depression ,It’s a theory and a bad one at that before you start your journey into Western psychology via big Pharma read a book called toxic psychology you might even question going into this profession if you have any morals
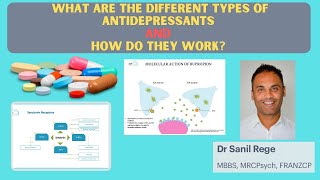
Finally someone that gone beyond the simple explanation that is an anthi histamine and in that way it help insomnia . Like this doctor explain it , also antagognice 5HT2C , like trazodone but without the QT alteration in the heart rytm like trazodone do. So it is really a good alternative to trazodone for that who cant stay asleep .
You are wrong my friend, on the contrary, it made a change in heart rhythm. Ventricular extrasystole is one of the most obvious side effects of mirtazapine, I experienced it.
Excellent presentation. Antidepressants are in general hit and miss, and carry a lot of social stigma. Explanations like this are very helpful to patients and their loved ones. Thank you.
Chemical imbalance in the brain is a theory for depression there is not one study that shows it causes depression these medication’s are evil if the doctor suggest some of them run don’t walk to find a new doctor
Fantastic explanation, I found this drug ticked every box for sever insomnia except for one main flaw, the next day fatigue and confusion became unbearable after 3 weeks on 15mg, was even starting to slur words , pity as it gave me a great sleep.
Yes it's the antihistaminergic effect for some. Theoretically increasing the dose reduces it but increasing dose is indicated in anxiety / depression. There are other agents that can also address insomnia - we have done a video in insomnia. How to Evaluate and Treat SLEEP PROBLEMS and INSOMNIA? - A Quick Guide | Psychiatrist Explains th-cam.com/video/Rrdx11rDa9o/w-d-xo.html
Thank you for making this video. I’ve recently been prescribed this medication and you explained what the drug itself does, in a way I could understand
Usually drugs that make you feel this good come with horrible side effects like severe constipation/urinary retention and movement disorders but mirtazipine has week anticholinergenic effects the worst thing is how dry my mouth feels sometimes but that's not a massive issue for me really this drug is so much better than sertaline
Weight gain and increased appetite are well known side effects. Both me and my sister and a neighbour all piled on the pounds when on it. I came off them a few years ago but have occasionally had one for insomnia when it's been bad 🌼
Life saver for me (15mg). I worry to much without Mirtazapine and I could not sleep for a year from stress. I'm 50 and also have sever ADHD. I will now use Mirtazapine for the rest of my life.
@@PieterPatrickMy eating pattern same my appetite is normal like before this medication but I am facing gastro problem and stomach bit pain after 10 days using this medicine how long to disappear these side effects??.How many days after starting Mirtazapine you get feel much better ? I started with 7.5 mg To day my 2nd week with 15 mg feeling drowsy and awful . 😔
I’ve just started Mirtazapine for emotional blunting and sexual dysfunction following Lexapro - currently on 15mg for week 1 - upping tomorrow to 30mg - cheerfully optimistic that there will be improvement. There are some encouraging studies
Not effective for OCD compared to SSRIs / Clomipramine and other augmentor. It may provide benefits for secondary OCD worsening mediated by depression and anxiety
I take this medication (15 mg) for two and a half months now together with my lithium, haldol and concerta. I sleep well and wake up with a clear mind and feel positive and happier. The anxiety is gone! Thank you for the clear explanation❤ Thank you sir
has anyone gone from mirtazapine to agomelatine? im just about to this and would like to see peoples feed back if they have done this :).. thank you so much for your video too. ive watched both your mirtazapine and agomelatine videos and its helped heaps understand more and stopped my worries about changing from 1 to another. I suffer from huge anxiety and left rehab 3 years ago (after 1.5 years in there) for ice/weed and alcohol addiction. So getting these meds right is crucial to me. Im an aussie so thank you with all your info!! :)
Yes it is a shift than can be done after discussion with the doctor. Agomelatine is now also TGA approved for Generalized anxiety disorder. One important point is that the last 15-7.5 mg of mirtazapine should be done very, very gradually as if done quickly or suddenly can lead to rebound insomnia / agitation. So in practice low dose mirtazapine can be kept for longer while agomelatine is optimised and then attempted to stop. This depends of course on if agomelatine treats insomnia and if insomnia is a feature of anxiety in first place. Ps not medical advice
What about deprel trazodone. Someone suggested me to after taper the mirtazapine 7.5 if I come on deprel trazodone it will help to come off from it then. I had really bad depression and anxiety and I have been using many different tabs and from last 1 and half year using mirtazapine 30mg and try to wean gradually but when I stopped after 5th night was hell 😢😢😢. I got reversed and again started to take back so now for 2 months I took 30mg and from last week taking 15mg. I hate taking these tabs or any tabs, doctors never help I made appointments for advice etc but nothing. I am not addicted to any drugs etc, my diet is healthy I walk support etc. If you will reply me back it will be big help ❤ Thanks in Advance
@@motherofprincesses5032 I finally just went cold turkey and took agomelatine straight away (it sucked) took 2 weeks to finally feel okay again and omg im sleep was aweful but agomelatine wasnt strong enough for my anxiety also my sleep sucked even after 2 months of taking it it wasnt like mirtazapine. The problem is im trying to find a med that doesnt numb my feelings because atm yes i feel good with my anxiety but due to this meds (or any meds) my relationship is copping it due to me not feeling as much and the sex life is fucked! Fukn mental health.
I got this for depression and to help me sleep. This makes me sleep perfect get atleast 10 hours but the next day when I'm at work I feel so tired and drained and feel like a zombie I'm only on 15mg
Yes, it has an anti histaminergic activity, which leads to sedation in the morning. Some people experience it more than others. In many cases, as tolerance to antihistaminergic activity increases with more prolonged use ( 3-4 weeks), this side effect should reduce. If it doesn't, and it affects daily activities, best discuss it with your doctor to consider the alternatives. Agomelatine is another agent that helps with sleep and is an antidepressant but does not lead to grogginess as it doesn't have antihistamine activity but instead has melatonin potentiation.
I had severe drowsiness when first taking it on just 7.5 mg. It was so bad that I had to cut it down to 3.75 mg. Now I’m up to 1/3 of a whole 15 mg tablet (5 mg). 😆
I increased from 15 to 30 two weeks ago and for the first time experience this side effect. I feel groggy and sleepy all day but at the same time feel more restlessness, especially in my hands.
Fantastic explanation! I'm on mirtazapine 15 mg for anxiety/depression only 1 week ago! I noticed a little improvement on anxiety but not in my mood. Should I wait a few weeks to see if it helps with mood? If I go up to 30 mg couldni have the risk that my anxiety got worse due to more noradreanline effects?
Thank you for your feedback. Can't give advice here. In general for mood and anxiety - 15-30 mg is needed - higher doses may be needed for depression. The anti histaminergic antagonism generally means that anxiety doesn't arisen - but can happen in some - dose adjustments then needed. Usually waiting 3-4 weeks for response is recommended before increasing dose. This is of course best discussed with your doctor who will individualise treatment for you.
I know 9 months has passed since this post for me this medication helped, although I put on 40kg I was wondering if you have had any symptoms like this. Thanks for sharing
Thank you for your videos; you are a gifted educator. I was suffering from sleep issues and severe anxiety and 8 months ago was prescribed Mirtazapine. I am very sensitive and had a range of physical ( deep fatigue at lower doses, jumpiness / heart palpitations at higher doses) and mental side effects (flashing kaleidoscope like dreams) as I went from 15mg up to 30mg. Sleep improved somewhat, and physical effects of anxiety such as adrenaline rushes and panic subsided, however unfortunately my cognitive anxiety has increased dramatically with obsessive fear, heightened apprehension about everything to where I am now incredibly psychologically fragile. I have been offered other medication to try, such as pregabalin, but am apprehensive about adding another possibly addictive medication to solve anxiety which may have been amplified by the Mirtazapine. On two days where I forgot to take the Mirtazpine, I have noted that I am a lot calmer, and this has me thinking that Mirtazapine might be the cause of my current heightened anxiety. I have casually asked the doctors about how to come off Mirtazapine, and they have mentioned that in their experience people can just stop taking it with little withdrawal symptoms - they seem unaware of any tapering schedules. Perhaps it is my anxiety speaking but I am concerned with withdrawal effects, as well as side effects at the different dosages noting that at the lower the dose the greater the sedation and fatigue (and less adrenaline effects) - and hence also how to transition to normal sleeping (if the lower dose is more sleep inducing) but at the same time, willing to stop the drug as soon as possible if it is causing issues. I wonder if you might be able to kindly recommend some common / sensible tapering schedules for this as well as any other ideas that I can discuss with my doctor. Many thanks in advance!
While we can’t give individual advice : in general if one is experiencing SE from a medication reduction and cessation will ease or stop the side effects. So Mirtazapine can be reduced to 15 mg for 4 days and then to 7.5 mg . It is this 7.5 mg cessation that can give an antihistaminergic rebound. For some patients they may need to be on this for a week or two before ceasing ; for others shorter or longer . One can only now by trying. During this period of cessation the doctor can prescribe another agent to treat the insomnia. This is general only and not medical advice. In general the shorter one has been on Mirtazapine the ‘easier’ it is to come off. However it is also important to identify the condition being treated - for mixed features ( video done) can be associated with worsening with antidepressants and presents with anxiety , hyperarousal , agitation. We also have a video on insomnia on the channel. Ps not medical advice. General only. Wish you well
Hi there again, Thank you so much for your very kind and informative reply ❤! Apologies for this but I wonder if you could please kindly clarify what you meant by “....worsening with antidepressants and presents with anxiety, hyperarousal and agitation”. Does that mean that Mirtazpine can cause such a response (anxiety, hyperarousal, agitation)? Thanks again 🙏♥
@@lcy_123 Antidepressant treatment is meant to improve activity, cognition and mood (experience of reward) without activating anxiety, or arousal in an ideal situation. When antidepressants worsen anxiety and increase arousal (restlessness, racing thoughts), this can be due to a mixed state (which is important to rule out) as ADs worsen mixed states. Your doctor will be able to discuss this more. We have a video on this. Search for mixed features.Any antidepressant can do this.
My psychiatrist said that he didn't think mirtazapine would have any more positive effect for depression or anxiety above 45mg, based on the studies he's seen. He also said at had to do with something being completely saturated. He has only ever had one patient on 60mg and he said it didn't help with the depression any more than the 45mg and it just Made him really hungry. In your clinical experience have you found doses of 45mg plus effective in different mental illnesses for people, if so what mental illness.
As mentioned in the video 45 mg and in some cases higher doses of 60 mg are needed for the dopaminergic effects. This may be the case in patients that have ultra rapid metabolism or rapid metabolism of the CYP enzymes that metabolise mirtazapine. Clinically 60 mg is used and in some rare cases 90 mg are seen in practice ( this is not recommended) as max doses are 45 or 60 mg depending on countries.
Also when thinking about doses it becomes more important to identify whvj symptoms are being targeted. If anhedonia and motivation is an issue then dopaminergic and NE enhancers are needed. Since mirtzapine is induced by 3 cyp enzymes - many patients being rapid metabolisers or smokers may need higher doses. A fixed dose of 30-45 mg in some patients may result in a sub therapeutic effect. psychscenehub.com/psychinsights/pharmacogenomics-drug-prescribing-psychiatry/
@@jaydavis1673 unlikely to do so as no poly aromatic hydrocarbons. But change from smoking to vaping could change drug concentrations as.smoking induction has stopped.
Hi I'm 58 and went on zoloft for panic attacks severe anxiety. I had awful side effects and horrendous withdrawal even tapering. I had a disassociation feeling which scares me to death. 5 months off still getting sweats chills. My gp have me mirtazapine 15mg for sleep and anxiety but .so scared to take because of the experience on zoloft and also prozac. Should I try this ? I've heard side effects aren't like ssri. I don't want weight gain , can it be kept off with low carb diet and exercise ?
Mirtazapine has better tolerability and can help with sleep and anxiety. Weight gain is a side effect ( doesn't occur in all patients) ; however if it occurs, diet, exercise and additional strategies are treatments for weight gain. There are alternative medication like agomelatine that have similar effects like mirtazapine but no weight gain and no withdrawal. Evidence-based for anxiety and can treat insomnia. P.S not medical advice psychscenehub.com/psychinsights/agomelatine-mechanism-action/
Hi doc, i take Bupropion and Guanfacine already and was suggested this for my insomnia by my provider. But wouldnt the mitrazapine effect on the a2 ports cancel out the effects of Guanfacine? Or does this happen only at doses higher than 15mg? Was suggested to start at 7.5mg for my sleep
lower doses do not have prominent alpha 2 A action. And it doesn't cancel out, it potentiates at higher doses. Mirtazapine is alpha 2 pre synaptic antagonist which does the ‘same’ ( re neurotransmitters) as a post synaptic alpha 2 A - guanfacine. Just that one is via presynaptic end ; other direct post synaptic
@@PsychiatrySimplifiedthank you for your reply, so helpful! I was hesitant after what i read online but this reassures me. Interesting, so even at 7.5mg it should potentiate the guanfacine effects or higher dosage are needed for alpha 2 effects?
Is it true that no doctor or psychiatrist can really prescribe any medication for a person unless a brain scan is performed to know the chemistry of the brain of their patients and not just throwing a medicine out hoping it works for the person? I was just on this medicine at 30 mg and it made me a slug and the night terrors was horrible but I have never been on medicine before and it was to treat my anxiety and depression but I stopped bc I don’t like how it makes me feel
I'm now in a process of withdrawal from Mirtazapine and it's terrbile. After 48h from the last dose the insomnia is back, i sleep 2-3 a night also feel very edgy and agitated 😢. However I feel less fatigued now than when I took the drug. I just hate how Mirtazapine makes you feel drowsy and fatigued all the time.
Sorry to hear. Mirtazapine reduction should be done gradually (mainly the last dose) as the last dose ceasing can lead to a antihistaminergic rebound. This rebound insomnia can be managed with other options which can be discussed with the doctor. However, it's important not to leave the severe insomnia untreated. Wish you well.
@@PsychiatrySimplified Thanks for the answer. At this stage I'm considering psychotherapy. Another thing that is I get very itchy skin rash in random places all over my body that comes and goes . It started when I quit Mirtazapine and gradually it's getting worse to the point my fingers are so swollen I can't grab any item. I already have a visit with my GP to try to fix the damn rash. It drives me nuts especially in the evenings.
wonderful explanation. I was prescribed 7.5 mg for sleep, to switch from benzos that l was using for over a week. It worked great but after about 7 days l stopped cold turkey because l did not understand that there is a withdrawal (my GP told me antidepressants are much lighter and cause no addiction) and l thought l was cured - l felt good, slept well and thought - allright, time to switch to naturals. Keep in mind that l never used any medicine before and had issues. 4th day after stopping, l plunged into severe withdrawal - insomnia, crying, doomlike feeling, completely out of whack, walking around with a massive pressure in my chest and unease. I was pretty surprised and googled it - figured it is discontinuation. My GP said no way, you have been less than 2 weeks on it. Okay, so l went a month without this med and this has been a TERRIBLE month. I resolved to benzo (sleeping pill or anti-anxiety) here and there to get at least some hours of sleep. After a month, l tested the hypothesis of differentiating withdrawal and rebound symptoms. So l took only a 2mg Mirtazapine before sleep. Slept 7 blissful hrs. Woke up without anxiety. Took the next day - even though l haven't slept well due to some worries , l was still absolutely normal and fine the next day - no crying, no doom, no sadness, no massive pressure in the chest. The next day, fine as well. Actually first time l felt normal. Now, how can a dose of 2-3 mg restore my normal emotional state if it is not withdrawal? So, to test it further, l discontinued after these 2 days and exactly 48 hrs later, l plunged into severe insomnia and 'woke up' with a massive chest pain and unease. Also crying. So, now l can't decide if l should reinstate and taper down slowly (my GP will think l am a hypochondriac) or just cruelly not take anything and persevere another month to see if l will be clean of withdrawal. I am asking this because l took Mirtazapine less than 2 weeks incrementally so l have a feeling that my withdrawal shouldn't be severe.
Thank you for sharing. There is one aspect to consider. The original reason. The causality works in the following way. Insomnia present ➡️medication prescribed ( gaba initially) ➡️ stopped ➡️ mild withdrawal gaba ➕original insomnia ➡️insomnia severity ⬆️ ( gaba not addressed by Mirtazapine ) Step 2. Mirtazapine prescribed after swap( anti H1) ➡️ insomnia treated Step 3 ➡️ Mirtazapine ceased ➡️ insomnia pre step 2 likely more in severity due to course and mild gaba withdrawal ➕antihistaminergic rebound ➡️ significant increase in severity ⬆️ ➡️ 2-3 mg addresing antihistaminergic rebound . But the severity of the insomnia is the missing piece. This is a common scenario where associations are made between medication and what comes after . But the original condition usually increases in severity ( insomnia usually does) over time which when combined with rebound or discontinuation phenomenon leads to a significant increase . The above is not set in stone and cannot be individualised to your personal situation. Also it is an hypothesis in general based on clinical presentations . Ps not medical advice.
Does Quetiapine hit the same receptors? My psychiatrist prescribed it to help with my mirtazapine withdrawal taper im scared to take incase I kindle my nervous system more.
Antihistaminergic withdrawal is the main issue with Mirtazapine. Quetiapine is a valid strategy that can help with tapering as it has antihistaminergic properties and allows for smaller dose reductions this assisting with any withdrawal symptoms
@@PsychiatrySimplified thank you im down to 3mg from 7.5 over 2 years im hypersensitive. Anxiety bad even with little drops. She said I can take as needed. Thanks for replying!
It is however really important to differentiate between withdrawal and return of anxiety as the original illness if that was something that was being treated .
Hi, I am starting mirtazipine next week, currently weening off sertraline after taking for 5 years. Can i ask what dose would be best to combat social anxiety and mild depression. My sleep hasnt been an issue. thanks
It depends. Often when medication is prescribed. It depends on the underlying symptoms that are being targeted and the other medications that may be prescribed together. For example, in some individuals mirtazapine at a low dose may assist with sleep in schizophrenia or bipolar disorder. However, it is more likely to do so, when an antipsychotic medication is already present as the primary pathophysiology and schizophrenia and bipolar disorder is to do with heightened dopaminergic potentiation. Thus in treatment, it becomes important to reduce the heightening of the dopaminergic system, and then a medication, such as Morteza peen, maybe prescribed to treat residual insomnia. Similarly, if mirtazapine is prescribed at higher doses in schizophrenia or bipolar disorder where prominent affect of symptoms are present. This could trigger of a manic or hypomanic episode. In summary, unopposed antidepressants are more likely to result in issues in bipolar disorder, rather than if a buffer with a mood stabiliser and/or antipsychotic is created. Similarly, mirtazapine can be prescribed in schizophrenia and there is evidence for this once the predominant psychotic symptoms are treated. Hope that makes sense. another important point is that in bipolar affective disorder or schizophrenia. The mechanism of insomnia is different hence It becomes important for the clinician to delve into the details of the nature of insomnia. For example, is it difficulty falling asleep versus difficulty staying asleep, waking up several times in the middle of the night, vivid dreams, or nightmares, versus early morning awakening. Each one of these has a different mechanism that needs to be targeted differently. Hence, an individualised approach to insomnia becomes necessary. You can see this described in the video that I did on insomnia on this channel.
Thank you for this great video. I do have a question. You mentioned that with higher doses that "mixed states" should be ruled out. Does this only apply to bipolar disorder, or a can a mixed state also refer to anxiety and depression symptoms that are occurring at the same time? Also, what doses would the mixed states caution typically apply to?
Thanks for the feedback and good question. A mixed state indicates a bipolar trait - does not necessarily mean bipolar disorder. It indicates the propensity for activation phenomenon with antidepressants. Anxiety and depression occurring together is not usually what is called a mixed state - but anxiety can be a feature in mixed states. We cover mixed state here in this video where we go into more detail. th-cam.com/video/hVMObsNmnf4/w-d-xo.html Usually doses of >30 mg but in some even lower doses can ‘activate them’. Hope this helps.
Doctor, I have problem waking up at early morning at 2:30am every day. i go to bed at 10pm and wake up at 2:30 am always, is it ok to take tab mirtaz 7.5 mg middle of my sleep at 2:30am so that I coul 0:13 d go back to sleep after 2:30am. Kindly advice me. Thank you 🙏
We can't provide advice here. Early morning awakening needs an evaluation to rule out agitation etc ; please discuss this with your doctor. Wish you well
Mirtazapine typically does not lead to akathisia - it’s also a treatment for akathisia . Akathisia has a strict definition of a subjective compulsion to move. Mirtazapine can lead to activation phenomenon - and at higher doses can potentially also lead to akathisia. Usually 5HT2A activation leads to akathisia ( Mirtazapine is an antagonist) . One key mechanism is the NAc ( nucleus accumbens shell part being activated through noradrenergic dysfunction ) Antipsychotic induced akathisia is multiple mechanisms How to Diagnose and Treat Akathisia (Antipsychotic Side Effect) - A Consultant Psychiatrist Explains th-cam.com/video/GBSTgSaLUsg/w-d-xo.html
Noreandrenergic dysfunction meaning an increase in norepinephrine? Would an alpha blocker be a suitable treatment. If one is already in an hypaepsusd state, would mirtazapine exacerbate they hyperaoused state even further ? Is there evidence of over stimulation of the locus coeruleus in akathisia?
@@jamescullen-657 Have a view of the video on akathisia. It's difficult to give yes, or no answers as symptoms have to be put in context of overall presentation.
Thanks for the reply Sanil. So it sounds like mirtazapine can cause restlessness due to activation of norepinephrine and dopamine? Can restlessness look similar to akathisia?
Thank you for your feedback. I’ve covered mechanisms overall - hoping it’s helpful Psychopharmacology of Selective Serotonin Re-uptake Inhibitors (SSRIs) - Mechanism of Action th-cam.com/video/bXFbDFPoiXE/w-d-xo.html
If the H1 receptor causes sleepiness and appetite stimulation at low doses does that mean weight gain is reduced at higher doses as it is for sleepiness? Great work!
Not necessarily. Theoretically it should but that’s not seen in clinical practice. As its 5HT2C antagonism also contributes to weight gain / metabolic aspects
Withdrawing from this is a nightmare. Currently 8 months off (was on a dose of 7.5 mg for 6 weeks only), for anxiety. Stopped taking it as it caused very blurry vision amongst other side effects. It did however help with appetite. While withdrawing I had most of the withdrawal symptoms. 8 months since stopping this med and still have Insomnia and Gastrointestinal issues which I never had before I was prescribed this!
One of the things that is important to recognise is that while withdrawal symptoms can occur the effects of the underlying illness need to be considered. Take an analogy - the medication puts a lid on the underlying symptoms so individuals get back to a level of functioning. When this lid is removed while withdrawal Sx are part of medication being tapered if the underlying illness was not in complete remission in for a period of time then this underlying illness Sx also come.up this exacerbating the overall picture. Generally individuals that have reached remission for a period of time can reduce and cease medication with withdrawals being manageable and time limited. There are always exceptions. But the key aspect is many look at it the medication side without recognising that underlying Sx of illness many be playing a part. Hence why it is important to discuss this with your doctor and get appropriate advice. Many individuals see the medication as a single factor but untreated or poorly treated anxiety or depression can continue to worseen in many which can preset with many different symptoms. Hence why it's important to consider a medical evaluation. Wish you well
@@PsychiatrySimplified I actually find this response very offensive and the reason the medication has not been labeled as causing these issues as the original comment or and myself as well as thousands of other people who took the time to write the same side effects online are clearly telling you the tablets cause these issues? Doctors are giving it to people for sleep issues! For anxiety! For depression! They don’t know they are highly addictive and cause life threatening issues!!!
@@EMPERORSPROTECTION-TERRA4LIFE Mirtazapine has a very low probability of serotonin syndrome ; doesn’t mean it can’t - but if it doesn’t happen in 100s of patients and happens in one individual then it can be indicative of certain factors that maybe associated - pharmacogenetics , neurobiology , associated agitation, nature of illness etc. causality is never straight forward . One if the criteria for causality is consistency . Why doesn’t serotonin syndrome occur in the majority of it is causal is the question to ask in clinical practice .
Doctor i was prescribed mirtaz 15 for my insomnia but it dinot work. So steooed upto 30 mg after a week.. At 30 mg iam sleeping well but daytime drowsiness is horrible, i cant function at all
I started taking mirtazapine in rehab while I was tapering off methadone, it really helped with sleep. That was 4 years ago, since I started taking it I have put on 40kg. Now I’m stressing about my weight and wanting to get off this medication but I’m scared of any withdrawal symptoms that may have to face. I’m just lost as to what to do ?
There are multiple options here. Have you discussed ethics with your doctor. They will be able to develop a plan specific to your needs. In general options include - ruling out medical causes, reduction of dose , switch to agent that doesn’t lead to weight gain ( withdrawal symptoms can be minimised) and /or augmentation with agents that result in weight loss. Many options available. Wish you well.
The antihistamine effect can lead to metabolic dysfunction , the 5 HT2C antagonism can lead to increase in appetite. The effect varies from person to person
@@jamescullen-657 depends. If intervened early temporary ; reversible. But if diabetes has developed - again in some can reverse but this depends on their risk factors as well ; genes, lifestyle , etc
Dr. Sanil thanks for the reply. I am confused because I have read that mirtazapine does not have a direct effect on glucose causing high blood sugars. What is the mechanism in which it can lead to diabetes? Do blood sugars need to be monitored on this medication if someone is not a diabetic?
Thank you for the video! I did want to put out a question to you. How similar does this drug potentially treat depression similarly to risperdal if they have any similarities? I was on risperdal for 3 months and it did help me quite a lot for depression but because of the side effects I had to come off and I wondered if this drug is a good alternative to risperidone in terms of treating depression though I am not schizophrenic or psychotic. If your wondering too I was on 0.5 on risperidone.
Risperidone is quite different from Mirtazapine. Risperidone has D2 antagonism and 5HT2A antagonism ( Mirtazapine also has 5HT2A antagonism). Mirtazapine has dose dependent effects as mentioned in the video - so there is a increase in DA & NA with higher doses - with higher doses risperidone reduces dopamine ( DA). Both can be used in depression but for different purposes. Mirtazapine lower doses mainly anti anxiety, higher doses to promote cognition , activity and mood. Risperidone is used in depression to reduce ruminative negative thoughts , agitation or over valued thoughts that are all consuming and negative. So it acts as an augmentation agent.
@@PsychiatrySimplifiedah okay that does make sense. That is probably why risperidone worked so well is because I do get ruminative negative thoughts and thought maybe this anti depressant would potentially do the same with those negative thoughts which have been a huge problem with my depression (my depression is persistent btw)
I've been left with permanent loss of libido due to sertraline.. It's not low, it's gone completely. I was recently prescribed Mirtazapine 15mg and it helped in that area when I first started. After about a week and a half, I went back to baseline. I strongly feel like I need a stronger dose. If Dopamine effects are seen at higher doses, I think a higher dose is what I need. I need to talk to my Doctor.. but am I wrong in this regard?
Thank you for providing a wonderful and informative video. I have been taking 3mg of lunesta for a few months for severe chronic insomnia for 3 years sleep hygiene, melatonin do not work. My Dr says I can try 7.5mg for my insomnia. Do you think Mirtazapine is better option for long term insomnia than Lunesta? Just worried about weight gain and next day sedation Thank you Sir
Lunesta works through GABA pathways. There can be a risk of dependence. Mirtazapine works through anti histaminergic action . Weight gain is a side effect. It also has anti depressant and anti anxiety properties. Newer agents for insomnia include suvorexant and lemborexant - orexin antagonist that are not associated with risk of dependence. In insomnia it is important to rule out other conditions and consider medication that is targeted. Your doctor will be in a better position to choose and explain. Wish you well.
I have recently tried 15mg, 30mg and now springing for 45mg. I heard that 45mg can reduce sedation and drowsiness. I did not know that this could be a combined with stimulants. I have ADD and so I have been prescribed stimulants in the past but they would trigger my anxiety too much and would have to stop. I am now wondering what is the optimal dose for me. If I could combine the two drugs together with a stimulants then maybe I could take lower doses and be able to manage the drowsiness that usually occurs next day.
You may want to look at the video on clonidine ad guanfacine which are used in combination with stimulants to manage or reduce anxiety. Ps not medical advice th-cam.com/video/TioM9NymZXc/w-d-xo.html
Hi Dr Rege , I have a question, does the Mirtazapine 5HT2A antagonism is responsible for increased DA and NE in prefrontal cortex or 5HT2C antagonism- Also activation of which one of them is linked to SSRI emotional blunting , kind regards Samuel Mansour GP , WA Perth
Thanks for the question. Both have effects in DA increase 5HT2 C and A but with Mirtazapine the DA increase also happens via a 5HT1A effect. 5HT2A is linked to emotional blunting. Hence Mirtazapine reducing this. But 5HT2C is exploited by Agomelatine to reduce emotional blunting. Vortioxetine does it via increase in DA and NA via multimodal mechanisms . Hope this help. If you are a GP interested in detailed education that’s RACGP accredited 👉academy.psychscene.com as it helps with showing these aspects via case studies
Hello, Doctor! I was prescribed Mirtazapine (15 mg) specifically for chronic nausea, vomiting, loss of appetite and weight loss. Had excellent results for all of those symptoms; my appetite is back, I haven't vomited since and I'm finally able to enjoy my meals again. But I'm having trouble with excessive drowsiness during the day, even with + 8 hours of sleep. Sleep was never a problem for me before taking the medication. Could increasing the dose to 30 mg or 45 mg counteract the drowsiness without losing the antiemetic and appetite-stimulating effects? Thank you so much!
This specific question is best answered by your doctor. In general however, if sedation is there but symptoms have settled - reduction of dose is one option. If symptoms return then a trial of increase may be considered.( here 30 mg can be significantly sedsting as well; 45 mg is meant to increase NA and DA to counteract sedation but this doesn't always happen) . Hence the steps above. Wish you well.
@@EMPERORSPROTECTION-TERRA4LIFE I've taken Mirtazapine for literally 15 years - no exaggeration. 14 days ago I split my dose in half. 7 days ago I stopped completely. THE MOST severe effect I could report on is marginally less heavy sleeping/sedation and marginally less appetite. Anti Depressant witch hunt nutters are the absolute worst, most confounding, saddest life wasters I've ever seen on the internet.
While taking another NaSSA (mianserin 10 mg) + sertraline 50 mg in May last year, I developed severe sleep-onset myoclonus which hasn't resolved despite discontinuing both drugs. I'd shake awake the moment I'm about to transition from wakefulness to sleep. Didn't have any sleep problems prior to starting the psych meds. Is there anything I can do to get rid of the myoclonus? Why does it persist this long? Any advice would be appreciated.
This is not an uncommon side effect. Mirtazapine another NASSA has a 28 % incidence of Restless legs . While we can’t provide specific advice in general - non cessation is usually due to a triggered sleep dysfunction which can be addressed by usually short term long acting clonazepam 1-2 weeks - which is also evidence based on rem sleep behaviour disorder and is usually the choice or clonidine which reduces rem sleep activation and increases deep sleep. However it is essential.l that underlying agitation is treated ( which may require longer duration of agents ) Here is a detailed review I wrote for references if needed. Please note this is not advice and any treatment should involve consideration of the underlying illness and an individualised risk benefit analysis. psychscenehub.com/psychinsights/neurobiology-sleep/
Not usually a first line treatment for OCD or neuropathic pain. It may help with sleep but there are other antidepressants indicated for OCD / pain. These are usually SNRIs as targeting noradrenaline is needed in pain Mx. Importantly however a full evaluation is needed to rule out other conditions and understand the nature, severity and type of symptoms before the appropriate treatment is implemented. Ps not medical advice. Wish you well
I've been taking 7.5 mg for 4 weeks and have recently started developing a tolerance to it for my insomnia. What would you suggest as a next step? I'm not sure if 15mg would help as it's been claimed that this dosage has less sedating effects.
It would be inappropriate to provide advice on this forum. There are several aspects to consider when treating insomnia. Your doctor is in the best position to answer this. Please view this video on evaluation of insomnia. th-cam.com/video/Rrdx11rDa9o/w-d-xo.html
Hey doc, great video. Question, I will ask psychiatrist. I take guanfacine 3mg for ADHD and Remeron 7.5mg for sleep. They work great. However is the alpha 2 effect canceling out the Intuniv? From my understanding.. At 7.5mg, probably not.. Too low of a dose for that effect. But I am not a doc. Thanks!!!
Thanks for the feedback. No it won’t. Mirtazapine is alpha-2 presynaptic anatagonist at higher doses ( increase NA and DA with potentiation on adrenergic and dopaminergic receptors . Guanfacine is more postsynaptic alpha 2 ( see video on Guanfacine - potentiates action on adrenergic receptors. So both will do the same potentiate. It’s because one is presynaptic other is postsynaptic. Presyanaptic receptors are autoreceptors ( inhibition) - so antagonism has opposite effect.
@@PsychiatrySimplified wow, that is brilliant. Thank you! I am a bit of a nerd (electronics engineer) but not in biochemistry or medicine, so it's all new to me. That pre/post explanation clears up a LOT of confusion. My experience so far is that they definitely do seem to work well together, at least with respect to 'turning down' the peripheral nervous system a bit it seems. I do also take Adderall. The guanfacine has virtually eliminated side-effects of the amphetamine, and really the only reason I'm on mirtazapine is sleep assistance. I really do feel like this is the first time in maybe 30 years in which I am on a drug combination that seems to be working. I have no side-effects. Guanfacine is a pretty interesting drug. I will check out the videos. Thanks again.
@@PsychiatrySimplified thank you very much. I have subscribed to the channel. One thing that I think is interesting to note, simply because I've never seen it ever mentioned, is that the guanfacine also fixed my Raynaud's and acrocyanosis, something that I've had my entire life (before Adderall, too). The color of my skin would concern me, and I saw a vascular surgeon, who said, not to worry it is just a cosmetic condition (benign). He said it is from "sensitive nerves", which sounded like an over simplification lol. I didn't think much of it. But years later, when I added the guanfacine to my ADHD treatment, I noticed within just a few days that for the first time in my entire life, my skin was normal color, not red or dusky blue. It is still normal color. It would seem to me that the guanfacine must be doing something to help modulate/moderate the signaling in that system. Anyway I just thought I'd share that, because it was so profound. Thanks again.
@@lisweetie1556 you raise a very good point. Yes clonidine or Guanfacine both are treatments for this. Dexamphetamine or Ritalin are both associated with Raynauds or worsening of it. Because they act on alpha adrenergic receptors associated with vasoconstriction and increase in peripheral vascular resistance - also increase BP due to this effect. Clonidine and Guanfacine both treat this. It is a side effect that can be overlooked but many complain of this. I always mention this in teaching. Thanks for sharing
I've been taking mirtazapin at a dose of 7,5 mg for almost a year now. It helps against my insomnia, I sleep longer and don't wake up as often. So far the only side effects are a hangover and increased appetite.
@@hypnotherapist2211 Drowsiness in the morning should get better over time, will take several weeks though. I still take the 7,5 mg dose, it works good for me personally, hangover is not so bad anymore. However I must exercise a lot to prevent getting overweight, I get so hungry especially late in the evening, that's a challenge sometimes.
@@ralfj.1740 so far I have been ok food wise if anything I have a loss of appetite and I am on 15mg . Thanks for answering . Praying that the tiredness wears off soon. I am only day 7 :)
I've been on mirtazapine 45mg for roughly 8 months have been on votiixetine for five weeks had some bad side effects so tapering of that now started sertraline 50mg today how long will it take to feel benafit from the sertraline
Depends on what were side effects ? Usually combination of Mirtazapine 45 mg and Vortioxetine increases DA and NA , if underlying hyperarousal is present then this can be worsened. Therefore a history of what has improved and what has worsened helps understand what the next steps are. It’s a balance between calming hyperarousal and I improving cognition and activity . So it’s not possible to predict for an individual unless a detailed history of symptoms is taken . Your doctor should be able to explain the duration of response . Wish you well . Ps not medical advice
would eating high histamine foods reverse the weight gain effect of Mirtazepine? I took Agomelatine that blocks 2c and didn't notice any weight gain or excess appetite so must be the antihistamines part that does it. I also had no activation/mixed symptoms unlike on ssri on that but equally no antidepressant effect after 10 wks. Why might that be? Am able to sleep okish and dr is only suggesting Mirtazapine for its 2a blocking effect for depression and anxiety(I had akathisia from Latuda so AP are out. Withdrawal of Abilify caused akathisia too years ago by different dr). I don't tolerate ssri, they cause anxiety/mixedness/akathisis not really sure what it is??!! There is bipolar in family and its well treated by VA+LAM+Prozac combo. My dr doesn't seem to understand mixedness can occur without being bipolar 1/2 yet the same bipolar meds are still used to treat it. She refuses to use mood stabilisers in me as saying its not bipolar. LAM with ssri did not stop mixedness and I want to try VA but she won't. She says my family member is likely being treated for a personality disorder rather than bipolar on that combo so I don't need those types of meds!! I have another psychiatrist lined up for a second opinion and will take your mixed features MDD info with me. This is all so frustrating....
I'm sorry to hear. Agomelatine is evidence based in bipolar depression and does not activate as it does not increase DA.or NA in the mesolimbic system which where the mixed features ( irritability ,Racing thoughts, hostility, anger dyscontrol etc occur). It does not have anti histaminergic action so no weight gain. eating foods with histamine does not reverse weight gain. In terms of antidepressant effect it is important to recognize that depression consists of 3 domains. Activity, cognition and emotion ( low mood and sadness - which is different from emotional lability - difficulty controlling emotions ( more related to mesolimbic). So when one wants an ‘antidepressant effect - the question is what specific symptoms are being targeted. Amotivation slowed movement ( activity dimensions - linked to dopamine and NA); cognition ( attention and concentration, decision making ) - linked to dopamine in the frontal lobe; cognition -Thoughts) - guilt, hopelessness, etc. - PFC - amygdala ( so here, one has to look at both intensity and severity as both frontal lobe and mesolimbic system to be addressed). Agomelatine is a mild dopaminergic agent. There is hierarchy.of dopaminergic and Norsdrenergic agents. Similarly - sleep - ruminations before sleep - frontal - limbic ; racing thoughts - mesolimbic ; waking up multiple times - hyper arousal ( NA driven) / nightmares - NA driven ; early morning waking ( mesolimbic). So essentially the symptoms provide better info to choose meds rather than a diagnosis which is a label that does not take into account individual symptoms. Importantly the fronto limbic system is also involved in trauma. In adhd also fronto-striato ( read movement area) - limbic - in females however the presentation can be with mood deregulation as the frontal lobe top down inhibition is not present adequately on the limbic system - hence can present like mixed states. Overall a history and formulation based on Sx provides a management plan This is educational only and not medical advice.
While we can’t give individual advice in general - there is no issue with the combination but olanzapine has a sedative effect and hence can lead to sedation during the day. It’s not usual to prescribe it in the day unless one has prescribed it night time already and one needs day time agitation control
Excellent video, thank you Doctor! I got this for depression, I don't have problem to sleep. This makes me sleep too much and a I feel tired during the day. I'm on 15mg and today is only my third day. Is this side effect gradually disappearing?
At low doses Mirtazapine has antihistaminergic effects and therefore can be sedating. This effect can reduce over time ( 1 wk) , or by increasing the dose where it be one’s more activating ( 45 or 60) . In some though this effect can worsen with increased doses. Your doctor should be able to explain the reasons for the choice and what to expect. Wish you well.
This drug was a major disappointment for me - I was on paroxetine for many years but switched to this with the promise of efficacy but also the lack of sexual dysfunction. I found no benefit at either 15 or 30mg and suspect that at 30mg my anxiety was worse. It also gave me restless legs quite badly and weight gain, the only benefit I had was good sleep but as my mental state worsened, this benefit waned considerably. You mentioned something about if the meso limbic system was activated this would be a reason not to use mirtazepine (or increase the does above 45mg?) out of interest - why is this?
Hi Dr. Rege, If a patient has taken mirtazapine long term (6 years or more) and they begin to not feel the sedated effects of the mirtazapine as strongly as they once did during the first year of taking mirtazapine, have the h1 receptors been completely desensitized?
Yes the histamine receptors tend to downregulate reducing the sedation. In some this may not happen to the extent they want leading to residual day time sedation. But overall they tend to ddownregulate. This is also the reason why sudden cessation is not receommded due to rebound up regulation - histaminergic rebound.
Thanks Sanil! Is down regulation reversible with abstinence of the medication? If so can h1 receptors completely re-sensitize to their original state prior to the usage of the medication?
If indicated for treatment of depression as part of bipolar depression. Generally antidepressants are not indicated as along term treatment as it can lead to cycling. Mirtazapine at low doses is used for sedation. But it depends - should be a question for the psychiatrist.
Is it possible that this medication can suppress or mask symptoms of suppressed or long term H. Pylori in regards to its effect of reducing gastric acid secretion and pepsin secretion?
@@PsychiatrySimplified so this could have a knock on effect on the efficacy and or behaviour of medications, example methylphenidates? SSRI's, in regards to absorbion, or hydrolysis?
@@PsychiatrySimplified Yes, but how could it have a side effect of mania, if it's a beta adrenergic blocker?. Like, how could that happen if it's job is to reduce adrenaline/norepinephrine activity in the body? Thanks!
@@Mishalalzahrani_ Mania is not a common side effect. But medication labels may list it. Propranolol can affect sleep as it reduces melatonin levels. this can indirectly trigger manic episodes if insomnia is severe.
It is generally medication that does not affect the heart. It can result in weight again which can affect cholesterol levels. It does not affect sodium and K levels: in the elderly > 65 yrs there is a small probability of a drop in Na levels.
@@youknowcrimedontpay9257 this can be counteracted or an alternative metabolically friendly antidepressant can be considered. Your doctor will be able to advise.









Ive been taking this medication for three years and it has been a lifesaver. I suffered from extreme anxiety, a sense of despair and gloom that no other medication had solved. It has helped enormously. It also helped me with debilitating insomnia. I take 30 mg every night and will likely be on it for the rest of my life. 54 year old male
Thank you for sharing! 🙏🏼
Wait till you start getting the issues! There highly addictive for one and I kept getting seratonin syndrome and nobody could tell me what the issue was!
@@EMPERORSPROTECTION-TERRA4LIFE no issues at all, nothing but benefits. I know about serotonin síndrome and that hasn’t been a problem. You may have taken something else in addition to mirtazapine to trigger that in the first place
@@pauls4923 😂 not at all! Read everybodies relies about the nightmare they are going through because of this addictive drug and how the doctor ignored the basic question to “explain why we need to wean off a non addictive drug?”.
It’s an addictive drug simple as that
@@EMPERORSPROTECTION-TERRA4LIFE it’s a drug that has been a complete and total lifesaver for me and for many others. I don’t care if it’s addictive if it’s going to relieve overwhelming anxiety and depression. Thank God I’ve found it! I’ll be on it til death.
Don’t usually comment but this was an amazing video. Finally someone that explains without explaining every word as if to a child.
Thank you for your feedback
Been on this medication for decades now for sleep. There is nothing else quite like it. I get regular and deep sleep with it and wake up refreshed.
That’s good to know. Thanks for sharing
Weight gained or not ??
I was prescribed this medication post army, it was great, then plateaued, the doc recently realised i was still on the 15mg, and now has upped it 45mg and i have to say. my everyday life has become SO much more releif for anxitey, focus, mood and apetite. Thank you for your referenece
That’s good to know!
What about side effects with 45mg ??
What about side effects
@@AyeshaKhan-ll7mwmadam man jis bhi video ka neeechy comment karti hon ya parhti hon vahan ap hoti han chahay vo koi British ho indian ho pakistani ho matlab ap bhi meri trha Sara din yahi karti han is ka ilava banda is halat main or kar bhi kia sakta hae 😭😭😭😭😭
@@taqihaider456 G JB Mai ye medicine use kr Rai ti to mai bhi asi hi ho gae ti q k me ne bhttt salo se Ecetelopram use kia ta . Lekin ab mujhe mere Dr ne Raxil Cr dya hai q k Mera weight gain ho Raha ta . AP tention na lo ap kch weeks use kr ly in Sha Allah thk ho jae gi . Or ye time lety hai anti depression tablets so plzz sabr se Kam ly or apny Dr ko follow kry or meditation hai U tube Mai search kr ly foggy brain Anxiety or depression ki kch time kry in Sha Allah bhtt behtr feel kry gi .
Thank you for sharing your knowledge!! I used this for insomnia and severe postpartum depression years ago with great results. Years later I went back on for insomnia and night sweats during menopause. Again with great results, a good nights sleep is finally with no night sweats. Your explanation gave me a clear picture of how the medicine works which no one ever explained before to me. I am off of it now and no withdrawal issues. Thank you again for sharing.
Thank you for your feedback 🙏🏼
Can I ask how long you were on it and what mg? Thanks 😊
Anna if you dont mind answering, what was your plan for withdrawal and how long were you on Mirtazepine? I am having problems with insomnia and worry about taking an antidepressant just for it, but seriously considering Mirtazepine
For someone who is studying for his psychiatry boards, this was immensely helpful in understanding the receptor roles. Thank you.
Thank you for your feedback 🙏
You do know that there’s not any proof whatsoever that a chemical imbalance causes depression ,It’s a theory and a bad one at that before you start your journey into Western psychology via big Pharma read a book called toxic psychology you might even question going into this profession if you have any morals
You are a very inspiring teacher!!
I only wish there were more professionals and health care experts to your level
Thank you for your feedback 🙏🏼
Finally someone that gone beyond the simple explanation that is an anthi histamine and in that way it help insomnia . Like this doctor explain it , also antagognice 5HT2C , like trazodone but without the QT alteration in the heart rytm like trazodone do. So it is really a good alternative to trazodone for that who cant stay asleep .
Thank you for your feedback. 🙏🏼
You are wrong my friend, on the contrary, it made a change in heart rhythm. Ventricular extrasystole is one of the most obvious side effects of mirtazapine, I experienced it.
❤
@@umutrgp9269 can I ask what mg you was taking for this side effect to happen?
Excellent presentation. Antidepressants are in general hit and miss, and carry a lot of social stigma. Explanations like this are very helpful to patients and their loved ones. Thank you.
Thank you for your feedback. Really appreciate it 🙏🏼
Chemical imbalance in the brain is a theory for depression there is not one study that shows it causes depression these medication’s are evil if the doctor suggest some of them run don’t walk to find a new doctor
Fantastic explanation, I found this drug ticked every box for sever insomnia except for one main flaw, the next day fatigue and confusion became unbearable after 3 weeks on 15mg, was even starting to slur words , pity as it gave me a great sleep.
Yes it's the antihistaminergic effect for some. Theoretically increasing the dose reduces it but increasing dose is indicated in anxiety / depression. There are other agents that can also address insomnia - we have done a video in insomnia. How to Evaluate and Treat SLEEP PROBLEMS and INSOMNIA? - A Quick Guide | Psychiatrist Explains
th-cam.com/video/Rrdx11rDa9o/w-d-xo.html
Your passion for teaching is commendable !
Thank you 🙏🏻
You are simply outstanding helping lay persons understand the complex science of psychiatric drugs. Thank you for your channel
Thank you for your feedback 🙏🏻
Thanks!
Thank you . Really appreciate it
Really detailed explanation. Excellent.
Thank you for your feedback 🙏🏻
Thank you for making this video. I’ve recently been prescribed this medication and you explained what the drug itself does, in a way I could understand
Thanks for these wonderful lectures Dr. Sanil, they are very helpful
Thank you for your feedback 🙏🏼
Usually drugs that make you feel this good come with horrible side effects like severe constipation/urinary retention and movement disorders but mirtazipine has week anticholinergenic effects the worst thing is how dry my mouth feels sometimes but that's not a massive issue for me really this drug is so much better than sertaline
Weight gain and increased appetite are well known side effects. Both me and my sister and a neighbour all piled on the pounds when on it. I came off them a few years ago but have occasionally had one for insomnia when it's been bad 🌼
Life saver for me (15mg).
I worry to much without Mirtazapine and I could not sleep for a year from stress.
I'm 50 and also have sever ADHD.
I will now use Mirtazapine for the rest of my life.
Any side effects like weight gain??
@AyeshaKhan-ll7mw Yes, a bit.
But I think because I eat more.
They say you'll gain weight as side effect, but also that you'll eat more.
@@PieterPatrickMy eating pattern same my appetite is normal like before this medication but I am facing gastro problem and stomach bit pain
after 10 days using this medicine how long to disappear these side effects??.How many days after starting Mirtazapine you get feel much better ? I started with 7.5 mg To day my 2nd week with 15 mg feeling drowsy and awful . 😔
I've learnt a lot from this video. Thank you.
Thank you for your feedback 🙏🏼
I’ve just started Mirtazapine for emotional blunting and sexual dysfunction following Lexapro - currently on 15mg for week 1 - upping tomorrow to 30mg - cheerfully optimistic that there will be improvement. There are some encouraging studies
Finally a clear and comprehensive explanation! Thank you so much for this ❤ is mirtazipine effective in the treatment of OCD alongside therapy?
Not effective for OCD compared to SSRIs / Clomipramine and other augmentor. It may provide benefits for secondary OCD worsening mediated by depression and anxiety
As mirtzapine is a 5HT1 agonist(like triptans), it can be benfecial for migraine prophylaxis too at low doses 🙏
Now I understand why I don't get bad headaches anymore...Thanks for sharing ❤️
so informative! Thank you.
Great presentation!
Excelente presentation, thanks!
Thank you for your feedback.
Super Awesome, I appreciate it, And learned so much from this short video, keep up the good work.
Thank you for your feedback 🙏🏼
I take this medication (15 mg) for two and a half months now together with my lithium, haldol and concerta.
I sleep well and wake up with a clear mind and feel positive and happier. The anxiety is gone!
Thank you for the clear explanation❤
Thank you sir
That's good to know! Thank you for sharing 🙏🏼
What about side effects I am seriously is it good for dpdr and brain fog
Thank you so much made it easy to understand
has anyone gone from mirtazapine to agomelatine? im just about to this and would like to see peoples feed back if they have done this :).. thank you so much for your video too. ive watched both your mirtazapine and agomelatine videos and its helped heaps understand more and stopped my worries about changing from 1 to another. I suffer from huge anxiety and left rehab 3 years ago (after 1.5 years in there) for ice/weed and alcohol addiction. So getting these meds right is crucial to me. Im an aussie so thank you with all your info!! :)
Yes it is a shift than can be done after discussion with the doctor. Agomelatine is now also TGA approved for Generalized anxiety disorder. One important point is that the last 15-7.5 mg of mirtazapine should be done very, very gradually as if done quickly or suddenly can lead to rebound insomnia / agitation. So in practice low dose mirtazapine can be kept for longer while agomelatine is optimised and then attempted to stop. This depends of course on if agomelatine treats insomnia and if insomnia is a feature of anxiety in first place. Ps not medical advice
I will do this thank you so much ❤
What about deprel trazodone. Someone suggested me to after taper the mirtazapine 7.5 if I come on deprel trazodone it will help to come off from it then. I had really bad depression and anxiety and I have been using many different tabs and from last 1 and half year using mirtazapine 30mg and try to wean gradually but when I stopped after 5th night was hell 😢😢😢. I got reversed and again started to take back so now for 2 months I took 30mg and from last week taking 15mg. I hate taking these tabs or any tabs, doctors never help I made appointments for advice etc but nothing. I am not addicted to any drugs etc, my diet is healthy I walk support etc.
If you will reply me back it will be big help ❤
Thanks in Advance
@@motherofprincesses5032 I finally just went cold turkey and took agomelatine straight away (it sucked) took 2 weeks to finally feel okay again and omg im sleep was aweful but agomelatine wasnt strong enough for my anxiety also my sleep sucked even after 2 months of taking it it wasnt like mirtazapine. The problem is im trying to find a med that doesnt numb my feelings because atm yes i feel good with my anxiety but due to this meds (or any meds) my relationship is copping it due to me not feeling as much and the sex life is fucked! Fukn mental health.
I got this for depression and to help me sleep. This makes me sleep perfect get atleast 10 hours but the next day when I'm at work I feel so tired and drained and feel like a zombie I'm only on 15mg
Yes, it has an anti histaminergic activity, which leads to sedation in the morning. Some people experience it more than others. In many cases, as tolerance to antihistaminergic activity increases with more prolonged use ( 3-4 weeks), this side effect should reduce. If it doesn't, and it affects daily activities, best discuss it with your doctor to consider the alternatives. Agomelatine is another agent that helps with sleep and is an antidepressant but does not lead to grogginess as it doesn't have antihistamine activity but instead has melatonin potentiation.
I had severe drowsiness when first taking it on just 7.5 mg. It was so bad that I had to cut it down to 3.75 mg. Now I’m up to 1/3 of a whole 15 mg tablet (5 mg). 😆
I increased from 15 to 30 two weeks ago and for the first time experience this side effect. I feel groggy and sleepy all day but at the same time feel more restlessness, especially in my hands.
@@erinn1730what are you feeling now I am are you recovered your anxiety
How are you now
Fantastic explanation! I'm on mirtazapine 15 mg for anxiety/depression only 1 week ago! I noticed a little improvement on anxiety but not in my mood. Should I wait a few weeks to see if it helps with mood? If I go up to 30 mg couldni have the risk that my anxiety got worse due to more noradreanline effects?
Thank you for your feedback. Can't give advice here. In general for mood and anxiety - 15-30 mg is needed - higher doses may be needed for depression. The anti histaminergic antagonism generally means that anxiety doesn't arisen - but can happen in some - dose adjustments then needed. Usually waiting 3-4 weeks for response is recommended before increasing dose. This is of course best discussed with your doctor who will individualise treatment for you.
Te fue bien? Tengo miedo de que me siente mal y me cree demasiada adicción, y me rompa las noches
@@javi.r.acosta lo siento. Trata de hablar con su doctor. Buena Suerte
I know 9 months has passed since this post for me this medication helped, although I put on 40kg I was wondering if you have had any symptoms like this. Thanks for sharing
@@deant6361 That's f up 40 kg oh nooooo
Very nice information. You are a great professor sir ❤❤
I love you so much from my heart.
Lots of love from me and my India
Thanks a lot🙏
Brilliant explanation as always Sanil..
Thanks you 🙏🏼
Thank you!! Very informative video 💯
Thank you for your feedback 🙏🏼
Thank you for your videos; you are a gifted educator. I was suffering from sleep issues and severe anxiety and 8 months ago was prescribed Mirtazapine. I am very sensitive and had a range of physical ( deep fatigue at lower doses, jumpiness / heart palpitations at higher doses) and mental side effects (flashing kaleidoscope like dreams) as I went from 15mg up to 30mg. Sleep improved somewhat, and physical effects of anxiety such as adrenaline rushes and panic subsided, however unfortunately my cognitive anxiety has increased dramatically with obsessive fear, heightened apprehension about everything to where I am now incredibly psychologically fragile. I have been offered other medication to try, such as pregabalin, but am apprehensive about adding another possibly addictive medication to solve anxiety which may have been amplified by the Mirtazapine. On two days where I forgot to take the Mirtazpine, I have noted that I am a lot calmer, and this has me thinking that Mirtazapine might be the cause of my current heightened anxiety. I have casually asked the doctors about how to come off Mirtazapine, and they have mentioned that in their experience people can just stop taking it with little withdrawal symptoms - they seem unaware of any tapering schedules. Perhaps it is my anxiety speaking but I am concerned with withdrawal effects, as well as side effects at the different dosages noting that at the lower the dose the greater the sedation and fatigue (and less adrenaline effects) - and hence also how to transition to normal sleeping (if the lower dose is more sleep inducing) but at the same time, willing to stop the drug as soon as possible if it is causing issues. I wonder if you might be able to kindly recommend some common / sensible tapering schedules for this as well as any other ideas that I can discuss with my doctor. Many thanks in advance!
While we can’t give individual advice : in general if one is experiencing SE from a medication reduction and cessation will ease or stop the side effects. So Mirtazapine can be reduced to 15 mg for 4 days and then to 7.5 mg . It is this 7.5 mg cessation that can give an antihistaminergic rebound. For some patients they may need to be on this for a week or two before ceasing ; for others shorter or longer . One can only now by trying. During this period of cessation the doctor can prescribe another agent to treat the insomnia. This is general only and not medical advice. In general the shorter one has been on Mirtazapine the ‘easier’ it is to come off. However it is also important to identify the condition being treated - for mixed features ( video done) can be associated with worsening with antidepressants and presents with anxiety , hyperarousal , agitation. We also have a video on insomnia on the channel. Ps not medical advice. General only. Wish you well
Hi there again, Thank you so much for your very kind and informative reply ❤! Apologies for this but I wonder if you could please kindly clarify what you meant by “....worsening with antidepressants and presents with anxiety, hyperarousal and agitation”. Does that mean that Mirtazpine can cause such a response (anxiety, hyperarousal, agitation)? Thanks again 🙏♥
@@lcy_123 Antidepressant treatment is meant to improve activity, cognition and mood (experience of reward) without activating anxiety, or arousal in an ideal situation. When antidepressants worsen anxiety and increase arousal (restlessness, racing thoughts), this can be due to a mixed state (which is important to rule out) as ADs worsen mixed states. Your doctor will be able to discuss this more. We have a video on this. Search for mixed features.Any antidepressant can do this.
@@PsychiatrySimplified Thanks once again for your kind and informative reply🙏
Should I be taking this medication for insomnia? I’m not depressed but cannot sleep. Was just prescribed this today.
Please discuss this with your doctor. Insomnia is not a single entity - there are different sleep phases - your doctor will be able to advise
Great video thank u
Thank you for your feedback
Thank you, cheers from Yekaterinburg
Thank you for your feedback 🙏🏻
My psychiatrist said that he didn't think mirtazapine would have any more positive effect for depression or anxiety above 45mg, based on the studies he's seen. He also said at had to do with something being completely saturated. He has only ever had one patient on 60mg and he said it didn't help with the depression any more than the 45mg and it just Made him really hungry. In your clinical experience have you found doses of 45mg plus effective in different mental illnesses for people, if so what mental illness.
As mentioned in the video 45 mg and in some cases higher doses of 60 mg are needed for the dopaminergic effects. This may be the case in patients that have ultra rapid metabolism or rapid metabolism of the CYP enzymes that metabolise mirtazapine. Clinically 60 mg is used and in some rare cases 90 mg are seen in practice ( this is not recommended) as max doses are 45 or 60 mg depending on countries.
Also when thinking about doses it becomes more important to identify whvj symptoms are being targeted. If anhedonia and motivation is an issue then dopaminergic and NE enhancers are needed. Since mirtzapine is induced by 3 cyp enzymes - many patients being rapid metabolisers or smokers may need higher doses. A fixed dose of 30-45 mg in some patients may result in a sub therapeutic effect. psychscenehub.com/psychinsights/pharmacogenomics-drug-prescribing-psychiatry/
@@PsychiatrySimplified thanks for the reply really appreciate it also if your smoking and need you more what about vaping?????
@@jaydavis1673 unlikely to do so as no poly aromatic hydrocarbons. But change from smoking to vaping could change drug concentrations as.smoking induction has stopped.
Hi I'm 58 and went on zoloft for panic attacks severe anxiety. I had awful side effects and horrendous withdrawal even tapering. I had a disassociation feeling which scares me to death. 5 months off still getting sweats chills. My gp have me mirtazapine 15mg for sleep and anxiety but .so scared to take because of the experience on zoloft and also prozac.
Should I try this ? I've heard side effects aren't like ssri. I don't want weight gain , can it be kept off with low carb diet and exercise ?
Mirtazapine has better tolerability and can help with sleep and anxiety. Weight gain is a side effect ( doesn't occur in all patients) ; however if it occurs, diet, exercise and additional strategies are treatments for weight gain. There are alternative medication like agomelatine that have similar effects like mirtazapine but no weight gain and no withdrawal. Evidence-based for anxiety and can treat insomnia. P.S not medical advice psychscenehub.com/psychinsights/agomelatine-mechanism-action/
Hi doc, i take Bupropion and Guanfacine already and was suggested this for my insomnia by my provider. But wouldnt the mitrazapine effect on the a2 ports cancel out the effects of Guanfacine? Or does this happen only at doses higher than 15mg?
Was suggested to start at 7.5mg for my sleep
lower doses do not have prominent alpha 2 A action. And it doesn't cancel out, it potentiates at higher doses. Mirtazapine is alpha 2 pre synaptic antagonist which does the ‘same’ ( re neurotransmitters) as a post synaptic alpha 2 A - guanfacine. Just that one is via presynaptic end ; other direct post synaptic
@@PsychiatrySimplifiedthank you for your reply, so helpful! I was hesitant after what i read online but this reassures me. Interesting, so even at 7.5mg it should potentiate the guanfacine effects or higher dosage are needed for alpha 2 effects?
Excellent video Sir by the way. Any studies done if mirtazapine lowers cortisol by increase in dopamine?
Is it true that no doctor or psychiatrist can really prescribe any medication for a person unless a brain scan is performed to know the chemistry of the brain of their patients and not just throwing a medicine out hoping it works for the person? I was just on this medicine at 30 mg and it made me a slug and the night terrors was horrible but I have never been on medicine before and it was to treat my anxiety and depression but I stopped bc I don’t like how it makes me feel
good 4 you
I'm now in a process of withdrawal from Mirtazapine and it's terrbile. After 48h from the last dose the insomnia is back, i sleep 2-3 a night also feel very edgy and agitated 😢. However I feel less fatigued now than when I took the drug. I just hate how Mirtazapine makes you feel drowsy and fatigued all the time.
Sorry to hear. Mirtazapine reduction should be done gradually (mainly the last dose) as the last dose ceasing can lead to a antihistaminergic rebound. This rebound insomnia can be managed with other options which can be discussed with the doctor. However, it's important not to leave the severe insomnia untreated. Wish you well.
@@PsychiatrySimplified Thanks for the answer. At this stage I'm considering psychotherapy.
Another thing that is I get very itchy skin rash in random places all over my body that comes and goes . It started when I quit Mirtazapine and gradually it's getting worse to the point my fingers are so swollen I can't grab any item. I already have a visit with my GP to try to fix the damn rash. It drives me nuts especially in the evenings.
Some people feel better reducing their serotonergic activity if their epigenetics express too little SERT
wonderful explanation. I was prescribed 7.5 mg for sleep, to switch from benzos that l was using for over a week. It worked great but after about 7 days l stopped cold turkey because l did not understand that there is a withdrawal (my GP told me antidepressants are much lighter and cause no addiction) and l thought l was cured - l felt good, slept well and thought - allright, time to switch to naturals. Keep in mind that l never used any medicine before and had issues. 4th day after stopping, l plunged into severe withdrawal - insomnia, crying, doomlike feeling, completely out of whack, walking around with a massive pressure in my chest and unease. I was pretty surprised and googled it - figured it is discontinuation. My GP said no way, you have been less than 2 weeks on it. Okay, so l went a month without this med and this has been a TERRIBLE month. I resolved to benzo (sleeping pill or anti-anxiety) here and there to get at least some hours of sleep. After a month, l tested the hypothesis of differentiating withdrawal and rebound symptoms. So l took only a 2mg Mirtazapine before sleep. Slept 7 blissful hrs. Woke up without anxiety. Took the next day - even though l haven't slept well due to some worries , l was still absolutely normal and fine the next day - no crying, no doom, no sadness, no massive pressure in the chest. The next day, fine as well. Actually first time l felt normal. Now, how can a dose of 2-3 mg restore my normal emotional state if it is not withdrawal? So, to test it further, l discontinued after these 2 days and exactly 48 hrs later, l plunged into severe insomnia and 'woke up' with a massive chest pain and unease. Also crying. So, now l can't decide if l should reinstate and taper down slowly (my GP will think l am a hypochondriac) or just cruelly not take anything and persevere another month to see if l will be clean of withdrawal. I am asking this because l took Mirtazapine less than 2 weeks incrementally so l have a feeling that my withdrawal shouldn't be severe.
lenghty, l mean. it is pretty hard to continue like this - oh and my tinnitus aggravated during withdrawal
Thank you for sharing. There is one aspect to consider. The original reason. The causality works in the following way. Insomnia present ➡️medication prescribed ( gaba initially) ➡️ stopped ➡️ mild withdrawal gaba ➕original insomnia ➡️insomnia severity ⬆️ ( gaba not addressed by Mirtazapine )
Step 2. Mirtazapine prescribed after swap( anti H1) ➡️ insomnia treated
Step 3 ➡️ Mirtazapine ceased ➡️ insomnia pre step 2 likely more in severity due to course and mild gaba withdrawal ➕antihistaminergic rebound ➡️ significant increase in severity ⬆️ ➡️ 2-3 mg addresing antihistaminergic rebound .
But the severity of the insomnia is the missing piece. This is a common scenario where associations are made between medication and what comes after . But the original condition usually increases in severity ( insomnia usually does) over time which when combined with rebound or discontinuation phenomenon leads to a significant increase .
The above is not set in stone and cannot be individualised to your personal situation. Also it is an hypothesis in general based on clinical presentations . Ps not medical advice.
your thoughts on combining with wellbutrin
Mirtazapine can be combined with Bupropion under psychiatric supervision for treatment of difficult to treat depression.
I use wellbutrin 150 for almost a month now. Remeron on and off for sleep. Is there better combinations?
Does Quetiapine hit the same receptors? My psychiatrist prescribed it to help with my mirtazapine withdrawal taper im scared to take incase I kindle my nervous system more.
Antihistaminergic withdrawal is the main issue with Mirtazapine. Quetiapine is a valid strategy that can help with tapering as it has antihistaminergic properties and allows for smaller dose reductions this assisting with any withdrawal symptoms
@@PsychiatrySimplified thank you im down to 3mg from 7.5 over 2 years im hypersensitive. Anxiety bad even with little drops. She said I can take as needed. Thanks for replying!
@@scotscub76 hope things go well. Good luck!
It is however really important to differentiate between withdrawal and return of anxiety as the original illness if that was something that was being treated .
@@PsychiatrySimplified I took it for sleep. And subsequently gained 3 stone!
Hi, I am starting mirtazipine next week, currently weening off sertraline after taking for 5 years. Can i ask what dose would be best to combat social anxiety and mild depression. My sleep hasnt been an issue. thanks
So if you have any kind of bipolar or schizophrenia etc you can’t take this even in low dose for severe insomnia?
It depends. Often when medication is prescribed. It depends on the underlying symptoms that are being targeted and the other medications that may be prescribed together. For example, in some individuals mirtazapine at a low dose may assist with sleep in schizophrenia or bipolar disorder. However, it is more likely to do so, when an antipsychotic medication is already present as the primary pathophysiology and schizophrenia and bipolar disorder is to do with heightened dopaminergic potentiation. Thus in treatment, it becomes important to reduce the heightening of the dopaminergic system, and then a medication, such as Morteza peen, maybe prescribed to treat residual insomnia. Similarly, if mirtazapine is prescribed at higher doses in schizophrenia or bipolar disorder where prominent affect of symptoms are present. This could trigger of a manic or hypomanic episode. In summary, unopposed antidepressants are more likely to result in issues in bipolar disorder, rather than if a buffer with a mood stabiliser and/or antipsychotic is created. Similarly, mirtazapine can be prescribed in schizophrenia and there is evidence for this once the predominant psychotic symptoms are treated. Hope that makes sense. another important point is that in bipolar affective disorder or schizophrenia. The mechanism of insomnia is different hence It becomes important for the clinician to delve into the details of the nature of insomnia. For example, is it difficulty falling asleep versus difficulty staying asleep, waking up several times in the middle of the night, vivid dreams, or nightmares, versus early morning awakening. Each one of these has a different mechanism that needs to be targeted differently. Hence, an individualised approach to insomnia becomes necessary. You can see this described in the video that I did on insomnia on this channel.
❤
Thank you for this great video. I do have a question. You mentioned that with higher doses that "mixed states" should be ruled out. Does this only apply to bipolar disorder, or a can a mixed state also refer to anxiety and depression symptoms that are occurring at the same time? Also, what doses would the mixed states caution typically apply to?
Thanks for the feedback and good question. A mixed state indicates a bipolar trait - does not necessarily mean bipolar disorder. It indicates the propensity for activation phenomenon with antidepressants. Anxiety and depression occurring together is not usually what is called a mixed state - but anxiety can be a feature in mixed states. We cover mixed state here in this video where we go into more detail. th-cam.com/video/hVMObsNmnf4/w-d-xo.html
Usually doses of >30 mg but in some even lower doses can ‘activate them’. Hope this helps.
Doctor, I have problem waking up at early morning at 2:30am every day. i go to bed at 10pm and wake up at 2:30 am always, is it ok to take tab mirtaz 7.5 mg middle of my sleep at 2:30am so that I coul 0:13 d go back to sleep after 2:30am. Kindly advice me. Thank you 🙏
We can't provide advice here. Early morning awakening needs an evaluation to rule out agitation etc ; please discuss this with your doctor. Wish you well
Dr Sanil,
How is mirtazapine induced akathisia different from antipsychotic induced akathisia?
Mirtazapine typically does not lead to akathisia - it’s also a treatment for akathisia . Akathisia has a strict definition of a subjective compulsion to move. Mirtazapine can lead to activation phenomenon - and at higher doses can potentially also lead to akathisia. Usually 5HT2A activation leads to akathisia ( Mirtazapine is an antagonist) . One key mechanism is the NAc ( nucleus accumbens shell part being activated through noradrenergic dysfunction ) Antipsychotic induced akathisia is multiple mechanisms How to Diagnose and Treat Akathisia (Antipsychotic Side Effect) - A Consultant Psychiatrist Explains
th-cam.com/video/GBSTgSaLUsg/w-d-xo.html
Noreandrenergic dysfunction meaning an increase in norepinephrine? Would an alpha blocker be a suitable treatment. If one is already in an hypaepsusd state, would mirtazapine exacerbate they hyperaoused state even further ? Is there evidence of over stimulation of the locus coeruleus in akathisia?
@@jamescullen-657 Have a view of the video on akathisia. It's difficult to give yes, or no answers as symptoms have to be put in context of overall presentation.
Thanks for the reply Sanil. So it sounds like mirtazapine can cause restlessness due to activation of norepinephrine and dopamine? Can restlessness look similar to akathisia?
@@jamescullen-657 Yes absolutely it can
Thanks for the video starting on 30 mg I hope it works
Best of luck!
Can we just say that mirtazapine is reversible effect or process to some action of ssri
like sexual dysfunction, emotional blunting.
Does the increase In dopamine through the two channels mentioned = antidepressant effect at least I think you mentioned two
Yes 5HT2A antagonism and alpha 2 presynaptic antagonism
Hi found this very helpful. Do you have similar video for citalopram. Benefits, Pharmacodynamics & Pharmacokinetics. Side effects
Thank you for your feedback. I’ve covered mechanisms overall - hoping it’s helpful Psychopharmacology of Selective Serotonin Re-uptake Inhibitors (SSRIs) - Mechanism of Action
th-cam.com/video/bXFbDFPoiXE/w-d-xo.html
If the H1 receptor causes sleepiness and appetite stimulation at low doses does that mean weight gain is reduced at higher doses as it is for sleepiness? Great work!
Not necessarily. Theoretically it should but that’s not seen in clinical practice. As its 5HT2C antagonism also contributes to weight gain / metabolic aspects
@@PsychiatrySimplified Thank you Doctor. So there’s no escaping the weight gain other than adding in glp1 or sglt2?🧐or maybe metformin?
Withdrawing from this is a nightmare. Currently 8 months off (was on a dose of 7.5 mg for 6 weeks only), for anxiety. Stopped taking it as it caused very blurry vision amongst other side effects. It did however help with appetite. While withdrawing I had most of the withdrawal symptoms. 8 months since stopping this med and still have Insomnia and Gastrointestinal issues which I never had before I was prescribed this!
One of the things that is important to recognise is that while withdrawal symptoms can occur the effects of the underlying illness need to be considered. Take an analogy - the medication puts a lid on the underlying symptoms so individuals get back to a level of functioning. When this lid is removed while withdrawal Sx are part of medication being tapered if the underlying illness was not in complete remission in for a period of time then this underlying illness Sx also come.up this exacerbating the overall picture. Generally individuals that have reached remission for a period of time can reduce and cease medication with withdrawals being manageable and time limited. There are always exceptions. But the key aspect is many look at it the medication side without recognising that underlying Sx of illness many be playing a part. Hence why it is important to discuss this with your doctor and get appropriate advice. Many individuals see the medication as a single factor but untreated or poorly treated anxiety or depression can continue to worseen in many which can preset with many different symptoms. Hence why it's important to consider a medical evaluation. Wish you well
Exactly the same issue with me aswell as finding out it was causing seratonin syndrome. Absolute nightmare
@@PsychiatrySimplified I actually find this response very offensive and the reason the medication has not been labeled as causing these issues as the original comment or and myself as well as thousands of other people who took the time to write the same side effects online are clearly telling you the tablets cause these issues? Doctors are giving it to people for sleep issues! For anxiety! For depression! They don’t know they are highly addictive and cause life threatening issues!!!
@@EMPERORSPROTECTION-TERRA4LIFE Mirtazapine has a very low probability of serotonin syndrome ; doesn’t mean it can’t - but if it doesn’t happen in 100s of patients and happens in one individual then it can be indicative of certain factors that maybe associated - pharmacogenetics , neurobiology , associated agitation, nature of illness etc. causality is never straight forward . One if the criteria for causality is consistency . Why doesn’t serotonin syndrome occur in the majority of it is causal is the question to ask in clinical practice .
@@PsychiatrySimplified 😂
Doctor i was prescribed mirtaz 15 for my insomnia but it dinot work. So steooed upto 30 mg after a week.. At 30 mg iam sleeping well but daytime drowsiness is horrible, i cant function at all
I started taking mirtazapine in rehab while I was tapering off methadone, it really helped with sleep. That was 4 years ago, since I started taking it I have put on 40kg. Now I’m stressing about my weight and wanting to get off this medication but I’m scared of any withdrawal symptoms that may have to face. I’m just lost as to what to do ?
There are multiple options here. Have you discussed ethics with your doctor. They will be able to develop a plan specific to your needs. In general options include - ruling out medical causes, reduction of dose , switch to agent that doesn’t lead to weight gain ( withdrawal symptoms can be minimised) and /or augmentation with agents that result in weight loss. Many options available. Wish you well.
Any video on quetiapine?
Please view this video on antipsychotics as a whole - th-cam.com/video/3vLSMZObXqE/w-d-xo.htmlsi=9H4WCT0tejouIRW4
I have a question - why exactly does it cause weight gain? Thank you.
Antihistaminergic action. Possibly 5HT2C antagonism also associated with increased appetite.
Does mirtazapine negatively affect metabolism? Does it sensitize fat cells?
The antihistamine effect can lead to metabolic dysfunction , the 5 HT2C antagonism can lead to increase in appetite. The effect varies from person to person
Thanks for the reply. Is this a temporary metabolic dysfunction once the medication has been stopped or can it be permanent?
@@jamescullen-657 depends. If intervened early temporary ; reversible. But if diabetes has developed - again in some can reverse but this depends on their risk factors as well ; genes, lifestyle , etc
Dr. Sanil thanks for the reply. I am confused because I have read that mirtazapine does not have a direct effect on glucose causing high blood sugars. What is the mechanism in which it can lead to diabetes? Do blood sugars need to be monitored on this medication if someone is not a diabetic?
@@jamescullen-657 anti histaminergic related weight gain and metabolic dysfunction.
Thank you for the video! I did want to put out a question to you. How similar does this drug potentially treat depression similarly to risperdal if they have any similarities? I was on risperdal for 3 months and it did help me quite a lot for depression but because of the side effects I had to come off and I wondered if this drug is a good alternative to risperidone in terms of treating depression though I am not schizophrenic or psychotic. If your wondering too I was on 0.5 on risperidone.
Risperidone is quite different from Mirtazapine. Risperidone has D2 antagonism and 5HT2A antagonism ( Mirtazapine also has 5HT2A antagonism). Mirtazapine has dose dependent effects as mentioned in the video - so there is a increase in DA & NA with higher doses - with higher doses risperidone reduces dopamine ( DA). Both can be used in depression but for different purposes. Mirtazapine lower doses mainly anti anxiety, higher doses to promote cognition , activity and mood. Risperidone is used in depression to reduce ruminative negative thoughts , agitation or over valued thoughts that are all consuming and negative. So it acts as an augmentation agent.
@@PsychiatrySimplifiedah okay that does make sense. That is probably why risperidone worked so well is because I do get ruminative negative thoughts and thought maybe this anti depressant would potentially do the same with those negative thoughts which have been a huge problem with my depression (my depression is persistent btw)
I've been left with permanent loss of libido due to sertraline.. It's not low, it's gone completely. I was recently prescribed Mirtazapine 15mg and it helped in that area when I first started. After about a week and a half, I went back to baseline. I strongly feel like I need a stronger dose. If Dopamine effects are seen at higher doses, I think a higher dose is what I need. I need to talk to my Doctor.. but am I wrong in this regard?
Thank you for providing a wonderful and informative video. I have been taking 3mg of lunesta for a few months for severe chronic insomnia for 3 years sleep hygiene, melatonin do not work.
My Dr says I can try 7.5mg for my insomnia.
Do you think Mirtazapine is better option for long term insomnia than Lunesta?
Just worried about weight gain and next day sedation
Thank you Sir
Lunesta works through GABA pathways. There can be a risk of dependence. Mirtazapine works through anti histaminergic action . Weight gain is a side effect. It also has anti depressant and anti anxiety properties. Newer agents for insomnia include suvorexant and lemborexant - orexin antagonist that are not associated with risk of dependence. In insomnia it is important to rule out other conditions and consider medication that is targeted. Your doctor will be in a better position to choose and explain. Wish you well.
@@PsychiatrySimplified thank you Dr may God Bless you
Can i take this with zoloft?
I have recently tried 15mg, 30mg and now springing for 45mg. I heard that 45mg can reduce sedation and drowsiness. I did not know that this could be a combined with stimulants. I have ADD and so I have been prescribed stimulants in the past but they would trigger my anxiety too much and would have to stop. I am now wondering what is the optimal dose for me. If I could combine the two drugs together with a stimulants then maybe I could take lower doses and be able to manage the drowsiness that usually occurs next day.
You may want to look at the video on clonidine ad guanfacine which are used in combination with stimulants to manage or reduce anxiety. Ps not medical advice
th-cam.com/video/TioM9NymZXc/w-d-xo.html
Seratonin syndrome is a common thing with this drug especially if you mix with other drugs
Hi Dr Rege , I have a question, does the Mirtazapine 5HT2A antagonism is responsible for increased DA and NE in prefrontal cortex or 5HT2C antagonism- Also activation of which one of them is linked to SSRI emotional blunting , kind regards Samuel Mansour GP , WA Perth
Thanks for the question. Both have effects in DA increase 5HT2 C and A but with Mirtazapine the DA increase also happens via a 5HT1A effect. 5HT2A is linked to emotional blunting. Hence Mirtazapine reducing this.
But 5HT2C is exploited by Agomelatine to reduce emotional blunting. Vortioxetine does it via increase in DA and NA via multimodal mechanisms . Hope this help. If you are a GP interested in detailed education that’s RACGP accredited 👉academy.psychscene.com as it helps with showing these aspects via case studies
@@PsychiatrySimplified thanks a lot
Hello, Doctor!
I was prescribed Mirtazapine (15 mg) specifically for chronic nausea, vomiting, loss of appetite and weight loss.
Had excellent results for all of those symptoms; my appetite is back, I haven't vomited since and I'm finally able to enjoy my meals again.
But I'm having trouble with excessive drowsiness during the day, even with + 8 hours of sleep. Sleep was never a problem for me before taking the medication. Could increasing the dose to 30 mg or 45 mg counteract the drowsiness without losing the antiemetic and appetite-stimulating effects?
Thank you so much!
This specific question is best answered by your doctor. In general however, if sedation is there but symptoms have settled - reduction of dose is one option. If symptoms return then a trial of increase may be considered.( here 30 mg can be significantly sedsting as well; 45 mg is meant to increase NA and DA to counteract sedation but this doesn't always happen) . Hence the steps above. Wish you well.
@@PsychiatrySimplified Thank you so much for your answer!
When you try and come off them you will regret ever taking them
@@EMPERORSPROTECTION-TERRA4LIFE I've taken Mirtazapine for literally 15 years - no exaggeration. 14 days ago I split my dose in half. 7 days ago I stopped completely. THE MOST severe effect I could report on is marginally less heavy sleeping/sedation and marginally less appetite. Anti Depressant witch hunt nutters are the absolute worst, most confounding, saddest life wasters I've ever seen on the internet.
@@goldmidwest ok so people who get wothdrawals are you saying they are lying?
While taking another NaSSA (mianserin 10 mg) + sertraline 50 mg in May last year, I developed severe sleep-onset myoclonus which hasn't resolved despite discontinuing both drugs. I'd shake awake the moment I'm about to transition from wakefulness to sleep. Didn't have any sleep problems prior to starting the psych meds.
Is there anything I can do to get rid of the myoclonus? Why does it persist this long? Any advice would be appreciated.
This is not an uncommon side effect. Mirtazapine another NASSA has a 28 % incidence of Restless legs . While we can’t provide specific advice in general - non cessation is usually due to a triggered sleep dysfunction which can be addressed by usually short term long acting clonazepam 1-2 weeks - which is also evidence based on rem sleep behaviour disorder and is usually the choice or clonidine which reduces rem sleep activation and increases deep sleep. However it is essential.l that underlying agitation is treated ( which may require longer duration of agents ) Here is a detailed review I wrote for references if needed. Please note this is not advice and any treatment should involve consideration of the underlying illness and an individualised risk benefit analysis. psychscenehub.com/psychinsights/neurobiology-sleep/
Mirtazapine certainly CAN cause emotional blunting. Although this is not necessarily a bad thing, it should be noted that it's commonly reported.
Can i take this as needed for sleep?
Can we take these as needed if we’re having a panic attack?
It is not prescribed in this manner.
Respected Sir
Is mirtazapine good for OCD and neuropathic pain.
I'm suffering from this😢
Not usually a first line treatment for OCD or neuropathic pain. It may help with sleep but there are other antidepressants indicated for OCD / pain. These are usually SNRIs as targeting noradrenaline is needed in pain Mx. Importantly however a full evaluation is needed to rule out other conditions and understand the nature, severity and type of symptoms before the appropriate treatment is implemented. Ps not medical advice. Wish you well
@@PsychiatrySimplified thank you sir for your suggestion ❤️
I've been taking 7.5 mg for 4 weeks and have recently started developing a tolerance to it for my insomnia. What would you suggest as a next step? I'm not sure if 15mg would help as it's been claimed that this dosage has less sedating effects.
It would be inappropriate to provide advice on this forum. There are several aspects to consider when treating insomnia. Your doctor is in the best position to answer this. Please view this video on evaluation of insomnia. th-cam.com/video/Rrdx11rDa9o/w-d-xo.html
Did any of you prescribed mitrazapine notice that it is a psychedelic drug?
In it's classical sense not classified as a psychedelic. What were the reasons you think it is? Curious?
@@PsychiatrySimplified why does my reply keep getting deleted?
@@psilocybe8135 which one ? Haven’t deleted any reply?
@@PsychiatrySimplified I wrote two detailed replies but they both vanished shortly afterwards.
Will try again.
@@psilocybe8135 weird
thank you!
Plz tell me is it cause of dpdr plz tell me about this medicine
Hey doc, great video. Question, I will ask psychiatrist. I take guanfacine 3mg for ADHD and Remeron 7.5mg for sleep. They work great. However is the alpha 2 effect canceling out the Intuniv? From my understanding.. At 7.5mg, probably not.. Too low of a dose for that effect. But I am not a doc. Thanks!!!
Thanks for the feedback. No it won’t. Mirtazapine is alpha-2 presynaptic anatagonist at higher doses ( increase NA and DA with potentiation on adrenergic and dopaminergic receptors . Guanfacine is more postsynaptic alpha 2 ( see video on Guanfacine - potentiates action on adrenergic receptors. So both will do the same potentiate. It’s because one is presynaptic other is postsynaptic. Presyanaptic receptors are autoreceptors ( inhibition) - so antagonism has opposite effect.
@@PsychiatrySimplified wow, that is brilliant. Thank you! I am a bit of a nerd (electronics engineer) but not in biochemistry or medicine, so it's all new to me. That pre/post explanation clears up a LOT of confusion. My experience so far is that they definitely do seem to work well together, at least with respect to 'turning down' the peripheral nervous system a bit it seems. I do also take Adderall. The guanfacine has virtually eliminated side-effects of the amphetamine, and really the only reason I'm on mirtazapine is sleep assistance. I really do feel like this is the first time in maybe 30 years in which I am on a drug combination that seems to be working. I have no side-effects. Guanfacine is a pretty interesting drug. I will check out the videos. Thanks again.
@@lisweetie1556 good to know that it’s working for you. Good luck and wish you well. Thanks for sharing.
@@PsychiatrySimplified thank you very much. I have subscribed to the channel. One thing that I think is interesting to note, simply because I've never seen it ever mentioned, is that the guanfacine also fixed my Raynaud's and acrocyanosis, something that I've had my entire life (before Adderall, too). The color of my skin would concern me, and I saw a vascular surgeon, who said, not to worry it is just a cosmetic condition (benign). He said it is from "sensitive nerves", which sounded like an over simplification lol. I didn't think much of it. But years later, when I added the guanfacine to my ADHD treatment, I noticed within just a few days that for the first time in my entire life, my skin was normal color, not red or dusky blue. It is still normal color. It would seem to me that the guanfacine must be doing something to help modulate/moderate the signaling in that system. Anyway I just thought I'd share that, because it was so profound. Thanks again.
@@lisweetie1556 you raise a very good point. Yes clonidine or Guanfacine both are treatments for this. Dexamphetamine or Ritalin are both associated with Raynauds or worsening of it. Because they act on alpha adrenergic receptors associated with vasoconstriction and increase in peripheral vascular resistance - also increase BP due to this effect. Clonidine and Guanfacine both treat this. It is a side effect that can be overlooked but many complain of this. I always mention this in teaching. Thanks for sharing
I've been taking mirtazapin at a dose of 7,5 mg for almost a year now. It helps against my insomnia, I sleep longer and don't wake up as often. So far the only side effects are a hangover and increased appetite.
Have you put weight on as any say
@@hypnotherapist2211 Yes I have but I'm working on it
@@ralfj.1740 has the drowsiness stopped. I ask as I am on day 7 and yesterday I could not get out of bed . And feel dizzy when I walk..
@@hypnotherapist2211 Drowsiness in the morning should get better over time, will take several weeks though. I still take the 7,5 mg dose, it works good for me personally, hangover is not so bad anymore. However I must exercise a lot to prevent getting overweight, I get so hungry especially late in the evening, that's a challenge sometimes.
@@ralfj.1740 so far I have been ok food wise if anything I have a loss of appetite and I am on 15mg . Thanks for answering . Praying that the tiredness wears off soon. I am only day 7 :)
Is it safe to combine with 10 mg citalopram? II cant tolerate ssris well, but low doses are not enough ...
Ps - not medical advice. Mirtazapine can be combined with SSRI. Of course, this should be discussed with the doctor.
I wish there was an alternative for sleep. This is nearly perfect for me however the food cravings make it tough.
There are many different options for sleep. Please check the video we did on Insomnia. th-cam.com/video/Rrdx11rDa9o/w-d-xo.html
Try exercise mirtazapine is garbage
I've been on mirtazapine 45mg for roughly 8 months have been on votiixetine for five weeks had some bad side effects so tapering of that now started sertraline 50mg today how long will it take to feel benafit from the sertraline
Depends on what were side effects ? Usually combination of Mirtazapine 45 mg and Vortioxetine increases DA and NA , if underlying hyperarousal is present then this can be worsened. Therefore a history of what has improved and what has worsened helps understand what the next steps are. It’s a balance between calming hyperarousal and I improving cognition and activity . So it’s not possible to predict for an individual unless a detailed history of symptoms is taken . Your doctor should be able to explain the duration of response . Wish you well . Ps not medical advice
would eating high histamine foods reverse the weight gain effect of Mirtazepine? I took Agomelatine that blocks 2c and didn't notice any weight gain or excess appetite so must be the antihistamines part that does it. I also had no activation/mixed symptoms unlike on ssri on that but equally no antidepressant effect after 10 wks. Why might that be? Am able to sleep okish and dr is only suggesting Mirtazapine for its 2a blocking effect for depression and anxiety(I had akathisia from Latuda so AP are out. Withdrawal of Abilify caused akathisia too years ago by different dr). I don't tolerate ssri, they cause anxiety/mixedness/akathisis not really sure what it is??!! There is bipolar in family and its well treated by VA+LAM+Prozac combo. My dr doesn't seem to understand mixedness can occur without being bipolar 1/2 yet the same bipolar meds are still used to treat it. She refuses to use mood stabilisers in me as saying its not bipolar. LAM with ssri did not stop mixedness and I want to try VA but she won't. She says my family member is likely being treated for a personality disorder rather than bipolar on that combo so I don't need those types of meds!! I have another psychiatrist lined up for a second opinion and will take your mixed features MDD info with me. This is all so frustrating....
I'm sorry to hear. Agomelatine is evidence based in bipolar depression and does not activate as it does not increase DA.or NA in the mesolimbic system which where the mixed features ( irritability ,Racing thoughts, hostility, anger dyscontrol etc occur). It does not have anti histaminergic action so no weight gain. eating foods with histamine does not reverse weight gain. In terms of antidepressant effect it is important to recognize that depression consists of 3 domains. Activity, cognition and emotion ( low mood and sadness - which is different from emotional lability - difficulty controlling emotions ( more related to mesolimbic). So when one wants an ‘antidepressant effect - the question is what specific symptoms are being targeted. Amotivation slowed movement ( activity dimensions - linked to dopamine and NA); cognition ( attention and concentration, decision making ) - linked to dopamine in the frontal lobe; cognition -Thoughts) - guilt, hopelessness, etc. - PFC - amygdala ( so here, one has to look at both intensity and severity as both frontal lobe and mesolimbic system to be addressed). Agomelatine is a mild dopaminergic agent. There is hierarchy.of dopaminergic and Norsdrenergic agents. Similarly - sleep - ruminations before sleep - frontal - limbic ; racing thoughts - mesolimbic ; waking up multiple times - hyper arousal ( NA driven) / nightmares - NA driven ; early morning waking ( mesolimbic). So essentially the symptoms provide better info to choose meds rather than a diagnosis which is a label that does not take into account individual symptoms. Importantly the fronto limbic system is also involved in trauma. In adhd also fronto-striato ( read movement area) - limbic - in females however the presentation can be with mood deregulation as the frontal lobe top down inhibition is not present adequately on the limbic system - hence can present like mixed states. Overall a history and formulation based on Sx provides a management plan
This is educational only and not medical advice.
Mirtazapine helped me who ever created this medication I wanna say Thank You❤️
Good to hear .
Is it good for dpdr and brain fog
Is it possible for mirtazapine to cause or exacerbate autonomic dysfunction (pots syndrome)?
No direct evidence - but if activation occurs - it is a possibility.
I have severe and intense panic attacks. What dosage of mirtazapine would you recommend? My doctor recommended 15mg
We can’t recommend or provide advice. In general Mirtazapine doses for anxiety are between 15-30 mg nocte. Wish you well
Can I take mirtaz 15 at night and olanzapine 2.5 at morning ?
While we can’t give individual advice in general - there is no issue with the combination but olanzapine has a sedative effect and hence can lead to sedation during the day. It’s not usual to prescribe it in the day unless one has prescribed it night time already and one needs day time agitation control
Excellent video, thank you Doctor! I got this for depression, I don't have problem to sleep. This makes me sleep too much and a I feel tired during the day. I'm on 15mg and today is only my third day. Is this side effect gradually disappearing?
At low doses Mirtazapine has antihistaminergic effects and therefore can be sedating. This effect can reduce over time ( 1 wk) , or by increasing the dose where it be one’s more activating ( 45 or 60) . In some though this effect can worsen with increased doses. Your doctor should be able to explain the reasons for the choice and what to expect. Wish you well.
@@PsychiatrySimplified thanks for your prompt reply! :)
@@PsychiatrySimplifieddoes the drug still work for insomnia and increased slow wave sleep once the antihistamine receptors down regulate?
This drug was a major disappointment for me - I was on paroxetine for many years but switched to this with the promise of efficacy but also the lack of sexual dysfunction. I found no benefit at either 15 or 30mg and suspect that at 30mg my anxiety was worse. It also gave me restless legs quite badly and weight gain, the only benefit I had was good sleep but as my mental state worsened, this benefit waned considerably.
You mentioned something about if the meso limbic system was activated this would be a reason not to use mirtazepine (or increase the does above 45mg?) out of interest - why is this?
Have a listen to this video as it will give an undertanding th-cam.com/video/UoS9WX83DIs/w-d-xo.htmlsi=Apbv_ikA1VY_-egr
Hi Dr. Rege,
If a patient has taken mirtazapine long term (6 years or more) and they begin to not feel the sedated effects of the mirtazapine as strongly as they once did during the first year of taking mirtazapine, have the h1 receptors been completely desensitized?
Yes the histamine receptors tend to downregulate reducing the sedation. In some this may not happen to the extent they want leading to residual day time sedation. But overall they tend to ddownregulate. This is also the reason why sudden cessation is not receommded due to rebound up regulation - histaminergic rebound.
Thanks Sanil! Is down regulation reversible with abstinence of the medication? If so can h1 receptors completely re-sensitize to their original state prior to the usage of the medication?
@@jamescullen-657 Yes. They can.
@@PsychiatrySimplifieddo the serotonin receptors that Mirtazapine block upregulate during long term treatment?
can mirtazapine at 15mg-30mg be used in conjunction with lithium and valprorate for bipolar disorder?
If indicated for treatment of depression as part of bipolar depression. Generally antidepressants are not indicated as along term treatment as it can lead to cycling. Mirtazapine at low doses is used for sedation. But it depends - should be a question for the psychiatrist.
What makes you gain weight, your appetite or the actual medication composition?
Medication mechanism plus individual vulnerability (genes, illness characteristics etc)
Is it possible that this medication can suppress or mask symptoms of suppressed or long term H. Pylori in regards to its effect of reducing gastric acid secretion and pepsin secretion?
Mask Symptoms it’s possible due to anti H1 and 5HT3 antagonism reducing GI effects.
@@PsychiatrySimplified so this could have a knock on effect on the efficacy and or behaviour of medications, example methylphenidates? SSRI's, in regards to absorbion, or hydrolysis?
@@joshuafuryon7874 No not in that sense.. Generally does not impact it to that extent like say a PPI would for some meds.
thank you :)@@PsychiatrySimplified
Can you take this medication with Clonazepam? I just got it prescribed to me today 15mg.
can propranolol increase noradrenaline in the CNS?
No. It’s a beta adrenergic blocker
@@PsychiatrySimplified Yes, but how could it have a side effect of mania, if it's a beta adrenergic blocker?. Like, how could that happen if it's job is to reduce adrenaline/norepinephrine activity in the body?
Thanks!
@@Mishalalzahrani_ Mania is not a common side effect. But medication labels may list it. Propranolol can affect sleep as it reduces melatonin levels. this can indirectly trigger manic episodes if insomnia is severe.
If the dose is like 1 mg does it reach the brain?
Yes it can.
Can mirtazapine cause problems to heart? I heard that is contributes to cholesterol level to go up as well sodium and potassium levels. Thank you
It is generally medication that does not affect the heart. It can result in weight again which can affect cholesterol levels. It does not affect sodium and K levels: in the elderly > 65 yrs there is a small probability of a drop in Na levels.
Interesting comment as my cholesterol level is up and so is my weight gain.
@@youknowcrimedontpay9257 this can be counteracted or an alternative metabolically friendly antidepressant can be considered. Your doctor will be able to advise.
M