Thanks! I know this video is over 5 years old. But based on all the other sources I’ve encountered, it filled in all the gaps, all the missing pieces. Too little importance is placed on knowing where the organs are located and the physical transports between them. Most grateful, Armando Hasudungan.
this is where it all comes down to when it comes to revising for exam times...... I'd honestly prefere to watch all your videos regarding my revision rather than going through some nonsense lecture slides which I didnt even attend for. I appreciate your hard work and your knowledge that you're sharing with us for free.... you couldn't be better..... I hope I'd find some videos to do with my final year as well......... cheeeeeeeers and big thank you.
This video smartly includes the co-locations of the organs and related transports (vessels, ducts, organs). That made it easier for my brain to understand the processes and biochemical triggers. And lastly at 11:05 This final explanation uses a linear timeline to restate all of it step-by-step. Basically, the same information restated in several ways always helps to answer questions and gaps in my comprehension. Based on the resources I’ve read or listened to, this video seems to be accurate. It uses several teaching aids: concise wording first, visuals (organs, etc), top level general and specifics diagrammed and finally as an action-based timeline. Worth subscribing to.
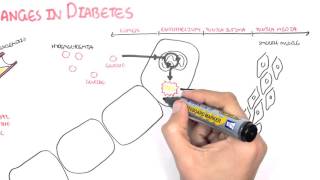
Insulin-dependent: GLUT 4- adipose tissue, striated muscle Insulin-independent: GLUT1- RBC, brain, cornea GLUT2- liver, beta-cells in the pancreas, kidney, small intestine GLUT3- Brain Ref: FIRST AID FOR THE USMLE STEP 1 2015
@@involuntarytwitch9771 yup sorry typo!. Glut 4 is the only Ins dependant for heart , skmuscle & adipose . Rest tissues Glucose move freely. However it's said that insulin somehow also has a fat sparing effect, don't know how exactly !
Hats off the way you present the content man....🙏🙏...I'm medico from India...And I'm glad to have mentor like you sir... Keep uploading.... Lots of love from India🇮🇳...❤️
me being a very slow learner i would take hours to understand little concepts but after your videos i have gained so much confidence in understanding critical concepts, thank you so much; may God Bless You.
This video is PERFECT (apart from the dodgy Glut-2 translocation thing which doesn't happen because of insulin since liver tissue is non-insulin dependant) But we know what u mean since it does happen with GLUT 4 in muscle and adipose. Apart from that this is so helpful. I love your videos, thanks for sharing them with us!
No words for your excellence You are making a topic very interesting and informative. I think I can pass my exams without reading whole the year but only watching ur videos on last night before exams 😁😀 Thank uhhhhh😘
little error: formation of prepro insulin as well as conversion of it to pro insulin by digestion of signal sequence by the help of enzyme endopeptidase ,both occurs in Endoplasmic reticulum only.then only it is budded of in the vesicle from the E.R. to reach golgi -apparatus,where again another endopeptidase separates c peptide from B-A segment(mature insulin)
I may be wrong but I think GLUT2, whilst mainly being expressed in the liver, is not insulin responsive in the way you described. GLUT2 channels have a high Km and so work with glucokinase in the liver to "sense" glucose levels (I think :P), but I don't think they respond to insulin...
Insulin stimulates glucokinase (not hexokinase) to create glucose-6-phosphate in the liver. Hexokinase is found in most tissues other than the liver and pancreatic beta cells. Correct?
Glucokinase is in the liver which phosphorylates glucose to G6P. In other tissues, such as adipose and muscles, it's hexokinase which phosphorylates glucose to G6P. So essentially yeah, you got it :)
Glucose uptake by liver is not insulin dependent. It's basically because of stimulation of hexokinase enzyme causing lack of intracytoplasmic glucose leading to facilitated diffusion of glucose via GLUT2 inside hepatocytes. Insulin doesn't play any role in increasing the GLUT2. Though it does increase GLUT 4 in adipose tissues, skeletal muscles and cardiac muscles.
FYI: Insulin upregulates GLUCOkinase, not HEXOkinase. Also, Insulin does not affect GLUT-2 in the liver and pancreas; GLUT-4 (in muscle and fat) is the only GLUT transporter that is insulin dependent.
A small point, but i believe the tyrosine kinase autophosphorylation occurs when the receptor is activated by insulin. It just seems like you suggest that they are always phosphorylated rather than when activated. Otherwise great video :D
You can use Ambrosia Blucon with Libre sensor and check your glucose values on your watch without even your phone in every 5 minutes. I check glucose values on my watch when my phone is not with me.
moshtarakman Insulin binds to tyrosine-kinase receptors in the adipose and skeletal muscle because their glucose is insulin dependent. This stimulates IRS-1, then GLUT 4 release from vesicles into the membrane. You are right. The GLUT 2 receptors are located in the pancreatic beta cells, liver, kidney and small intestine. They are insulin independent. Therefore, binding of Insulin to tyrosine kinase is not necessary. From my understanding. The insulin independent glucose transporters, such as GLUT 2, GLUT 1, and GLUT 3 are always there and are not unregulated or down regulated. Correct me if I'm wrong.
MedEdCYP450 Correct. I wouldn't go as far as saying that the non-insulin dependent GLUT receptors (1,2, and 5) are not regulated - they probably are regulated (depending on pathology) but you are right in that they are not regulated by insulin. Just a recap in case anyone needed it When sugar is high (after a meal), glucose can bind to non-insulin GLUT receptors. When glucose binds to GLUT2 on the B-cells of the pancreas, it induces insulin secretion. Insulin's main role is to prevent hyperglycemia. The big tissues that can really uptake glucose are skeletal tissue and adipose tissue but they can only take up glucose if they have GLUT4 expressed - only insulin can accomplish this upregulation. So what happens? Insulin binds to skeletal and adipose tissue's tyrosine kinase receptor. This causes two things to happen. First, it upregulates GLUT4 onto those tissues to allow glucose enter (and thus prevent hyperglycemia). The second thing it does is within those cells, it increases glycogen, protein, and lipid synthesis - this makes sense because the insulin wants to use up all the glucose to prevent hyperglycemia and so glucose gets used up to drive fat, protein, and glycogen synthesis.
moshtarakman I would like to add to this conversation that GLUT2 has a low affinity for glucose, which means it will only be "stimulated" or rather "accept" glucose in high levels. This makes perfect sense when it comes to the pancreas. The GLUT2 will only be stimulated after a meal (when you have high glucose levels) and thus release insulin, but as soon as the glucose levels diminish it won't be stimulated anymore due to it's low affinity. This is (probably) the reason why insulin is not released at normal P-glucose levels. EDIT: To clarify, GLUT1 and GLUT3 does NOT have a low affinity for glucose, they work just as well as GLUT4 but are insulin independent. Correct me if I'm wrong.
Isn't it glucokinase that is activated by insulin?Also was going to comment on GLUT4 being the transporter that is insulin dependent in muscle and adipose tissue. GLUT 2 is in the liver but not insulin dependent for anyone watching currently.
yeah ur right, liver uses GLUT 2 which is non-insulin dependant. but insulin does everything in this guys explanation in the liver but the translocation bit. The translocation thing happens in adipose and muscle though as they use GLUT 4 :)
I did not know that insulin stimulated the uptake of glucose to liver? I thought that insulin just stimulated the uptake of glucose via GLUT 4, and not GLUT 2 (in liver) :)
GLUT4 is in the muscle and adipose tissues, so a low insulin level would trigger the translocation of GLUT4 from vesicles intracellularly, to the cell membrane. The GLUT4 then fuse to the membrane and allow a rapid increase of glucose uptake into the cell. GLUT2 is associated with the liver
Wow, these videos are of really great quality! Although I don't study these topics in English, your articulation is so clear I have no problem understanding what you say. Subbed.
Hi Armando. i really appreciate your videos. You are doing a fantastic job. Maybe you should explain the difference between GLUT2 transporters (insulin independant) and GLUT4 (insulin dependant).
Super video thanks.What happened if stomack produce massive acidity? How is effective to pancreas the cells and insulin in for example as protein? s-s connection? ph in this area? Thanks
QUESTION: In the absence of blood glucose while in a state of ketosis (where glycogen stores in the liver and skeletal muscles are depleted), will the insulin increase caused by PROTEIN result in protein being shuttled into cells as fat, in which case what is the process by which this protein would be converted into fat?
Very informative. Thanks for sharing this and now I will share with people that don't think type 1 diabetes is a very serious disease. I'm hoping there is a cure someday even if it's not in my lifetime but just so so many people don't have to suffer anymore. Also hoping for a cure for type 2 diabetes both diseases are so terrible and lead to all kind of other diseases.
There is some complex mechanism involving internalization and regeneration of insulin receptor. I thought you have explained that too, but you have not explained it. :(
My pancreas levels were 115 last time got blood work. Dr was worried. Says 75 is normal. What are the symptoms of a bad pancreas? My kidney has been hurting the past week. Should I be worried it’s my pancreas sending bad amounts of insulin?









📌MAKE THIS LECTURE STICK: FREE PRACTICE QUESTIONS HERE! 🎓
youmakr.ai/test-playground/questionnaire/673d542a859b9c170836f2b7
Thanks! I know this video is over 5 years old. But based on all the other sources I’ve encountered, it filled in all the gaps, all the missing pieces. Too little importance is placed on knowing where the organs are located and the physical transports between them. Most grateful, Armando Hasudungan.
this is where it all comes down to when it comes to revising for exam times...... I'd honestly prefere to watch all your videos regarding my revision rather than going through some nonsense lecture slides which I didnt even attend for. I appreciate your hard work and your knowledge that you're sharing with us for free.... you couldn't be better..... I hope I'd find some videos to do with my final year as well......... cheeeeeeeers and big thank you.
8 years later your work is still helping all of us so much. You're a gem. God bless you.
You just saved my 5 hours studying physiology and biochemistry thanks!!!
You sometimes make me think that I can learn more on youtube than at school. And I don't even pay gas to get to youtube...
you pay internet bills
Obviously... Most of your teachers are bored and often quite dumb...
@@nayomayo603 internet bills! Lol! Who cares about 3$-5$
Also, a teacher can hardly draw a circle nicely, not to mention this kind of graphics!
This video smartly includes the co-locations of the organs and related transports (vessels, ducts, organs). That made it easier for my brain to understand the processes and biochemical triggers. And lastly at 11:05 This final explanation uses a linear timeline to restate all of it step-by-step. Basically, the same information restated in several ways always helps to answer questions and gaps in my comprehension.
Based on the resources I’ve read or listened to, this video seems to be accurate. It uses several teaching aids: concise wording first, visuals (organs, etc), top level general and specifics diagrammed and finally as an action-based timeline.
Worth subscribing to.
Insulin-dependent:
GLUT 4- adipose tissue, striated muscle
Insulin-independent:
GLUT1- RBC, brain, cornea
GLUT2- liver, beta-cells in the pancreas, kidney, small intestine
GLUT3- Brain
Ref: FIRST AID FOR THE USMLE STEP 1 2015
יעל רובה thankyou!
GLuT 4 is the only one which is Independent of Insulin..allows free movement of Glucose.
Isn't this backward? Glut-4 is insulin INDEPENDENT, whilst the others are all dependent?
@@involuntarytwitch9771 yup sorry typo!. Glut 4 is the only Ins dependant for heart , skmuscle & adipose . Rest tissues Glucose move freely. However it's said that insulin somehow also has a fat sparing effect, don't know how exactly !
Beta cells in the pancreas have actually GLUT1. GLUT2 is only in mice and rats and not in humans.
You are an excellent teacher. Thank you for the class.
you are a hero. thank you so much. i've never thought learning medicine would be easy
it changes a lot , for better of course , than the woman with no degree teaching endocrinology at my university ! Thanks a lot
Hats off the way you present the content man....🙏🙏...I'm medico from India...And I'm glad to have mentor like you sir...
Keep uploading....
Lots of love from India🇮🇳...❤️
me being a very slow learner i would take hours to understand little concepts but after your videos i have gained so much confidence in understanding critical concepts, thank you so much; may God Bless You.
GREAT work! I've been glued to textbooks and lecture notes trying to sort out everything involved with CHO metabolism, and this video was SO helpful!
This video is PERFECT (apart from the dodgy Glut-2 translocation thing which doesn't happen because of insulin since liver tissue is non-insulin dependant) But we know what u mean since it does happen with GLUT 4 in muscle and adipose. Apart from that this is so helpful. I love your videos, thanks for sharing them with us!
Thanks so much I am french and for me your video are the best one and the easiest to understand to learn biology in english;
I just really want to thank you for the clear and informative video. You are making medical school easy for me.
I have my exam next month and these videos are surely gonna help me! Thank you for making these topics fun to understand!!!
You never stop getting surprised about Armando's pedagogic skills !!!!!!!!!!!
Super
saving me hours of reading books and not understanding Mr. Hasudungan. Cheers!
No words for your excellence
You are making a topic very interesting and informative.
I think I can pass my exams without reading whole the year but only watching ur videos on last night before exams 😁😀
Thank uhhhhh😘
I used to drop out when it gets too detailed, but these vids are a really helpful quick overview and keep me going (: Thank you!
Thank you,Your videos are the assets for the medical student as they are excellent and free!
Thanks alot 👍
Lots of support and love from Pakistan
little error: formation of prepro insulin as well as conversion of it to pro insulin by digestion of signal sequence by the help of enzyme endopeptidase ,both occurs in Endoplasmic reticulum only.then only it is budded of in the vesicle from the E.R. to reach golgi -apparatus,where again another endopeptidase separates c peptide from B-A segment(mature insulin)
Yupp!
it really do helps me in understanding more about insulin mechanism of action. thanks a lot!!
Great way to understand the role of insulin. I have type 1 diabetes so good to know in so much detail.
I may be wrong but I think GLUT2, whilst mainly being expressed in the liver, is not insulin responsive in the way you described. GLUT2 channels have a high Km and so work with glucokinase in the liver to "sense" glucose levels (I think :P), but I don't think they respond to insulin...
Thank You so very much... You have no Idea how much I appreciate this video
Well presented and clear, making understanding easy. Excellent.
You are great !! Thank you very much , we even watch your videos from the other side of the world. From saudi arabia ❤️❤️❤️
Insulin stimulates glucokinase (not hexokinase) to create glucose-6-phosphate in the liver. Hexokinase is found in most tissues other than the liver and pancreatic beta cells. Correct?
Glucokinase is in the liver which phosphorylates glucose to G6P. In other tissues, such as adipose and muscles, it's hexokinase which phosphorylates glucose to G6P.
So essentially yeah, you got it :)
Its not very complicated.....glucose is a hexose sugar....and thus hexokinase or glucokinase are terms used interchangeably
finally understood the insulin receptor functions... genial artist!!!
Watching this at x2. I have an exam this morning and I'm going to ace it🔥
And this is how I avoid getting up early in order to attend pointless lectures of 1 hour at the university. 10 min youtube videos is the way to go XD
May God bless you:"(!!! U always save me with ur very very very very useful vedios Thaaaank youuuu
I love how i can draw these illustrated diagrams along with the theory explained. Thanks for the help.
Glucose uptake by liver is not insulin dependent. It's basically because of stimulation of hexokinase enzyme causing lack of intracytoplasmic glucose leading to facilitated diffusion of glucose via GLUT2 inside hepatocytes. Insulin doesn't play any role in increasing the GLUT2. Though it does increase GLUT 4 in adipose tissues, skeletal muscles and cardiac muscles.
You have helped me alot thank you so much !!! You’re videos are amazing as well as your drawings and your explanation.. thank you from my heart
i'm just in love with the scientific artist you are.
FYI: Insulin upregulates GLUCOkinase, not HEXOkinase. Also, Insulin does not affect GLUT-2 in the liver and pancreas; GLUT-4 (in muscle and fat) is the only GLUT transporter that is insulin dependent.
Great as always. I passed immunology with your videos and got A this summer. Thank you ❤️
Glucose uptake by the liver is actually not insulin-dependent...
Super! you help me understand deeply the mechanism of action which I thought I'd already known
Excellent work. Very professional and accurate.
autophosphosphorylation does not means that the tyr kinase is always phosphorylated!
but the rest is great ! ty
fantastic! youre helping me with my exam!
No. THANK YOU! Subscribed to this AMAZING CHANNEL. I hope you get all the support!
that is amazing ... when i do not understand any thing ,u help a lot ... thanks
very2 contributive, made our revision so much effective and easy, thanks a million sir
How do complex carbohydrates with little to no simple carbohydrates affect insulin production and use by cells?
You are totally amazing
Cannot get any better ,, truly magnificent
Best explanation so far.. Thankyou So Much
A small point, but i believe the tyrosine kinase autophosphorylation occurs when the receptor is activated by insulin. It just seems like you suggest that they are always phosphorylated rather than when activated. Otherwise great video :D
Armando u make amazing videos..it has helped me in my entire medicine course. 💙💛💙💛💙💕♥✔
You can use Ambrosia Blucon with Libre sensor and check your glucose values on your watch without even your phone in every 5 minutes. I check glucose values on my watch when my phone is not with me.
Insulin DOES NOT stimulate GLUT2 receptors - only GLUT4.
moshtarakman Insulin binds to tyrosine-kinase receptors in the adipose and skeletal muscle because their glucose is insulin dependent. This stimulates IRS-1, then GLUT 4 release from vesicles into the membrane.
You are right. The GLUT 2 receptors are located in the pancreatic beta cells, liver, kidney and small intestine. They are insulin independent. Therefore, binding of Insulin to tyrosine kinase is not necessary. From my understanding. The insulin independent glucose transporters, such as GLUT 2, GLUT 1, and GLUT 3 are always there and are not unregulated or down regulated. Correct me if I'm wrong.
MedEdCYP450 Correct. I wouldn't go as far as saying that the non-insulin dependent GLUT receptors (1,2, and 5) are not regulated - they probably are regulated (depending on pathology) but you are right in that they are not regulated by insulin. Just a recap in case anyone needed it
When sugar is high (after a meal), glucose can bind to non-insulin GLUT receptors. When glucose binds to GLUT2 on the B-cells of the pancreas, it induces insulin secretion. Insulin's main role is to prevent hyperglycemia. The big tissues that can really uptake glucose are skeletal tissue and adipose tissue but they can only take up glucose if they have GLUT4 expressed - only insulin can accomplish this upregulation. So what happens?
Insulin binds to skeletal and adipose tissue's tyrosine kinase receptor. This causes two things to happen. First, it upregulates GLUT4 onto those tissues to allow glucose enter (and thus prevent hyperglycemia). The second thing it does is within those cells, it increases glycogen, protein, and lipid synthesis - this makes sense because the insulin wants to use up all the glucose to prevent hyperglycemia and so glucose gets used up to drive fat, protein, and glycogen synthesis.
moshtarakman I would like to add to this conversation that GLUT2 has a low affinity for glucose, which means it will only be "stimulated" or rather "accept" glucose in high levels. This makes perfect sense when it comes to the pancreas. The GLUT2 will only be stimulated after a meal (when you have high glucose levels) and thus release insulin, but as soon as the glucose levels diminish it won't be stimulated anymore due to it's low affinity.
This is (probably) the reason why insulin is not released at normal P-glucose levels.
EDIT: To clarify, GLUT1 and GLUT3 does NOT have a low affinity for glucose, they work just as well as GLUT4 but are insulin independent. Correct me if I'm wrong.
+salmjak your comment is Sooooo quite thanks I really enjoyed
moshtarakman yeah u r ri8
Thanks for your useful video. One remark: GLUT2 (of liver) is insulin-Independent!
Love your videos. Saved my ass in exams time and time again.
The explanation is excellent, greeting from Mexico :)
Isn't it glucokinase that is activated by insulin?Also was going to comment on GLUT4 being the transporter that is insulin dependent in muscle and adipose tissue. GLUT 2 is in the liver but not insulin dependent for anyone watching currently.
very well explained kindly also make a video on its pharmacolgy
yeah ur right, liver uses GLUT 2 which is non-insulin dependant. but insulin does everything in this guys explanation in the liver but the translocation bit. The translocation thing happens in adipose and muscle though as they use GLUT 4 :)
well done I like the way you share with us! Can you write clearly the words next time, may be bigger size
amazing map and vids, you rock man
im so glad u covered insulin resistance :') my lecture notes were confusing. thank u!
I did not know that insulin stimulated the uptake of glucose to liver? I thought that insulin just stimulated the uptake of glucose via GLUT 4, and not GLUT 2 (in liver) :)
GLUT4 is in the muscle and adipose tissues, so a low insulin level would trigger the translocation of GLUT4 from vesicles intracellularly, to the cell membrane. The GLUT4 then fuse to the membrane and allow a rapid increase of glucose uptake into the cell.
GLUT2 is associated with the liver
Wow, these videos are of really great quality! Although I don't study these topics in English, your articulation is so clear I have no problem understanding what you say. Subbed.
Hi Armando. i really appreciate your videos. You are doing a fantastic job. Maybe you should explain the difference between GLUT2 transporters (insulin independant) and GLUT4 (insulin dependant).
isn't GLUT 2 insulin independent? - idk i maybe wrong but thanks the videos are great overall
You are the best
2022 still your videos are useful
Tnx🇦🇫😍🙏
Very well done explanation. I learn a lot.
Super video thanks.What happened if stomack produce massive acidity? How is effective to pancreas the cells and insulin in for example as protein? s-s connection? ph in this area? Thanks
Disulphide bonds in A chain too.
Because of you I wouldn’t think that I am stupid student 🤩
wow! soooo beautiful and perfect work!! THANKS to share with us. I love it =D
outstanding work
Brilliant video, thank you. Question is insulin necessary to synthese protein for muscles?
You are the best explainer
QUESTION: In the absence of blood glucose while in a state of ketosis (where glycogen stores in the liver and skeletal muscles are depleted), will the insulin increase caused by PROTEIN result in protein being shuttled into cells as fat, in which case what is the process by which this protein would be converted into fat?
Good stuff, thank you Sir!
Very informative. Thanks for sharing this and now I will share with people that don't think type 1 diabetes is a very serious disease. I'm hoping there is a cure someday even if it's not in my lifetime but just so so many people don't have to suffer anymore. Also hoping for a cure for type 2 diabetes both diseases are so terrible and lead to all kind of other diseases.
This is very awesome 👌.
informative one thanks a lot &great job
Thank you very much ❤️
Amazing videos, thanks a lot!
Very helpful , thank you so much
thankuuuuuuu soo much.. very helpful it is😊
but liver doesnt hve GLUT4, instead it contains only GLUT2.
you r providing good understanding videos but please do little corrections in this video
Please make any video on functions of pineal gland
I don't find very clear about it even on TH-cam
You are just love sir❤️
There is some complex mechanism involving internalization and regeneration of insulin receptor. I thought you have explained that too, but you have not explained it.
:(
great video..but i think insulin has no effect on hexokinase....it is glucokinase that is under the influence of insulin
nicely explained. thank you very much for this.
So, what can I do for Diabetes? I am not going to take pharmaceuticals. Right now I am eating low carb. My glucose went from over 200 to 150.
I have chronic high insulin with normal glucose levels. I also have poor appetite when high insulin is supposed to increase appetite. I'm weird. :)
very good video ,thanks
love you videos but a little too fast... suggestion slow down just a bit with the fast writing and voice overs
Thanks again for posting
My pancreas levels were 115 last time got blood work. Dr was worried. Says 75 is normal. What are the symptoms of a bad pancreas? My kidney has been hurting the past week. Should I be worried it’s my pancreas sending bad amounts of insulin?